
Abstract

A 16-year-old African American male with a medical history of asthma and atopic dermatitis presented to our institution with a 2-month history of pain in his left mandible and ear as well as left temporal headache. He was recently seen at urgent care and referred to a dental clinic for a presumptive diagnosis of an infected, impacted tooth but was never seen in clinic. Review of systems was pertinent for trismus, odynophagia, weight loss, fever, and chills. Nasal endoscopy revealed a mass in the left nasopharyngeal space. A maxillofacial computed tomography (CT) scan was performed to further characterize the mass. Computed tomography showed a large left nasopharyngeal mass extending to the infratemporal region, with associated bony erosion and effacement of the left jugular vein and occlusion of the left internal carotid artery (ICA), later confirmed via magnetic resonance angiography (Figure 1) and venography (Figure 2). Magnetic resonance imaging (MRI) of the face and base of the skull demonstrated an invasive soft tissue mass in the left nasopharyngeal area extending to the retropharyngeal spaces, the skull base, and left temporomandibular joint (Figure 3A and B). Biopsy revealed an Epstein-Barr virus (EBV) + nasopharyngeal carcinoma (NPC) type 2, nonkeratinizing, undifferentiated. After careful consideration of the affected anatomy, the surgical team recommended chemotherapy with radiation. Our patient completed 3 cycles of chemotherapy with consolidation radiotherapy, and currently awaits clinical follow-up.

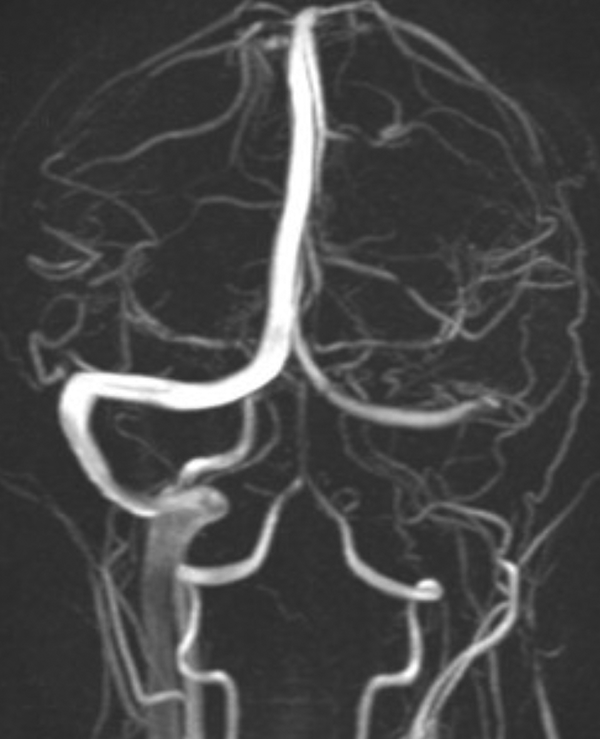
Magnetic resonance angiography (MRA): Coronal projection reveals occlusion of the left internal carotid artery.
Magnetic resonance venography: Coronal projection shows occlusion/compression of the left sigmoid sinus and internal jugular vein.
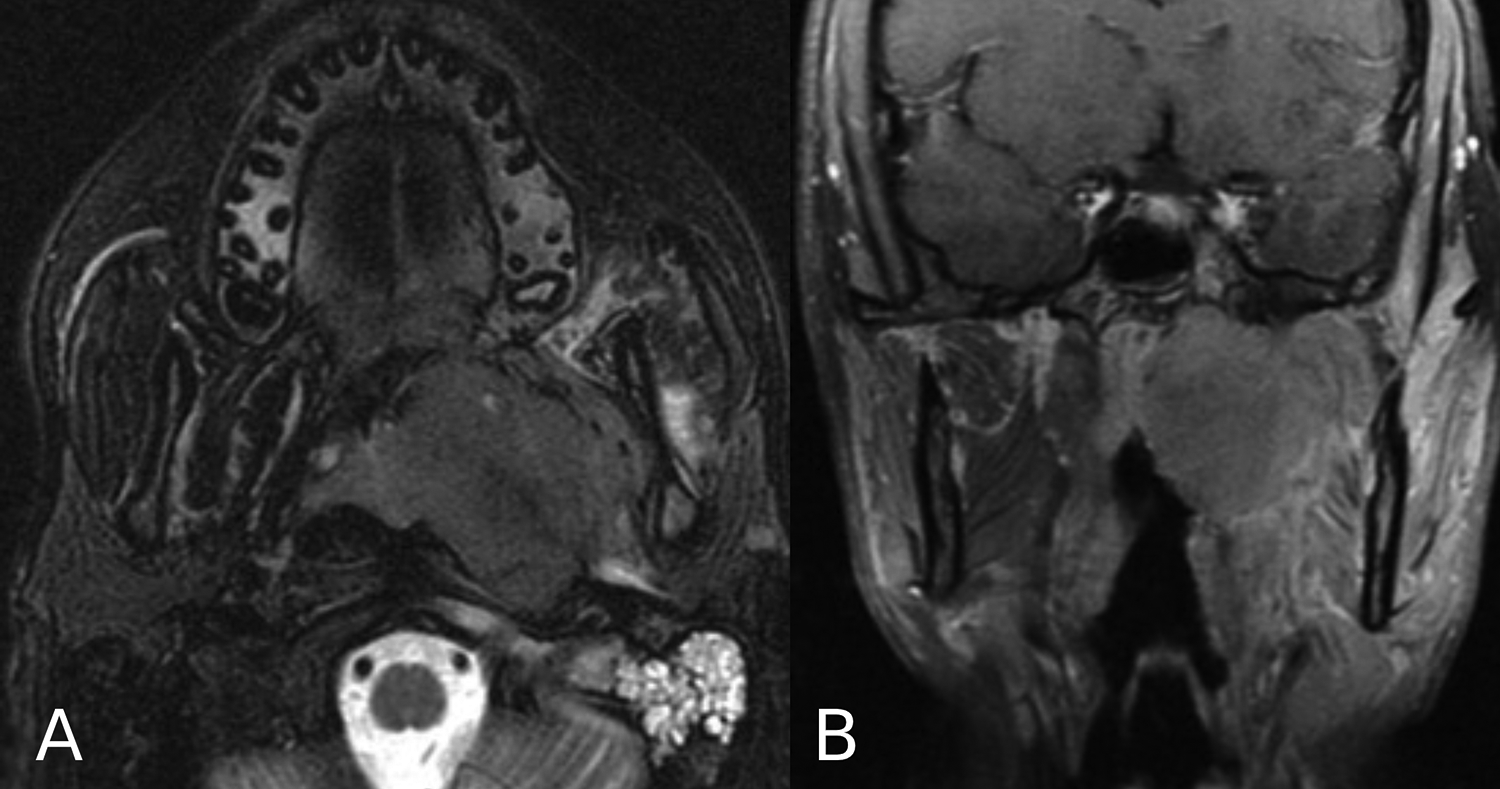
Magnetic resonance imaging (MRI) (A) axial T2W and (B) coronal T1 post-contrast images: Large invasive nasopharyngeal mass on the left, extending into the infratemporal and masticator spaces and left temporomandibular joint. Note: Fluid in the left mastoid air cells as a reflection of obstruction of the Eustachian Tube.
Nasopharyngeal carcinoma is a cancer of epithelial origin that arises from the nasopharyngeal mucosa. 1 The World Health Organization classifies this cancer into 3 pathological subtypes: keratinizing squamous, nonkeratinizing, and basaloid squamous. Nonkeratinizing NPC is further classified into differentiated and undifferentiated. 2 The nonkeratinizing type of NPC is the most common in endemic areas and is primarily associated with EBV infection. 3
Nasopharyngeal carcinoma is an uncommon tumor in the pediatric population, making up less than 1% of all childhood cancers. 2 Nasopharyngeal carcinoma has an uneven distribution worldwide; the incidence of NPC in pediatric populations in Europe and North America is low, approximating 1 per million, whereas endemic regions such as Southeast Asia have incidence rates approximating 1 to 20 per hundred thousand. 4 The symptomatology of NPC depends on the involved anatomy. 5 Most pediatric cases report a neck mass with possible nasal bleeding or discharge, otalgia, unilateral conductive hearing loss, headaches, and cranial nerve deficits. 2
Although NPC is primarily diagnosed via endoscopy with subsequent biopsy, cross-sectional imaging is crucial to tumor staging and often part of the initial workup. 5 CT imaging augments characterization by delineating invasion of bony structures, and reveals lytic or sclerotic lesions with cortical thickening, particularly involving the base of the skull. 6 Magnetic resonance imaging has been found to be superior for identification of submucosal or obscure mucosal lesions, which can appear normal on endoscopy. 7 Tumors are defined on MRI by low signal intensity on T1, intermediate signal intensity on T2, and increased enhancement relative to normal mucosal tissue following contrast. 7 Magnetic resonance imaging can assess parapharyngeal extension and cervical chain nodes and is thus central to primary and nodal staging. 6 Unilateral obliteration of the internal carotid fat separation plane on MRI defines tumor involvement of the carotid space. 2 Whereas most cases of NPC are commonly complicated by post-radiation ICA stenosis, 8 this case is notable in that our patient’s initial presentation involved complete occlusion of the right ICA, a phenomenon not yet described.
Of interesting note is the rarity of this cancer outside of endemic areas, particularly in pediatric populations. 1 In North America, given that the incidence of NPC averages < 1 per million in pediatric patients, risk factors play a crucial role in increasing the physician’s index of suspicion. It is well studied that those of Southern Chinese race-ethnicity are at highest risk of developing NPC. 4 Other demographics at increased risk include indigenous people of North Africa, Alaska, and South-East Asia. 4 Epstein-Barr virus is classically associated with undifferentiated NPC which is also the most common subtype in pediatric cases. 7 Of note, lower socioeconomic status is associated with a higher risk of NPC. 2 This connection is thought to be due, in part, to the association of increased consumption of preserved foods and decreased consumption of fresh fruit and vegetables, both conferring an increased risk of NPC. 2 An intimate understanding of their patient population is paramount to the physician in guiding diagnosis, as it can increase one’s index of suspicion of this rare entity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.