
Abstract
Objectives:
Our study was aimed at finding a definitive treatment protocol for the management of sudden sensorineural hearing loss (SSNHL) and to study the prognostic factors affecting it.
Methods:
This randomized clinical study was conducted on a total of 150 patients. All patients older than 10 years and presenting within 15 days of experiencing the symptom of SSNHL and with no known etiology were included. Patients were divided into 2 groups. In group I patients, we administered systemic steroids (injection dexamethasone 3 days, followed by oral deflazacort for 6 days) with liquid glycerol; and in group II, we administered systemic steroids alone (injection dexamethasone 3 days, followed by oral deflazacort for 6 days). The total time for which the treatment was instituted was 9 days and patients were assessed on the basis of their pure tone audiogram and speech discrimination score done at days 0, 3, 7, 21, and 42.
Results:
There were 77 males and 73 females. Vertigo (P value < .00) and diabetes mellitus (P value < .001) had a negative prognostic influence on the recovery rate in both the groups. The comparison revealed that group I (DG) in which patients received injection dexamethasone with oral glycerol had a higher recovery rate of 86.7% as compared to group II (D) patients, in which patients received injection dexamethasone alone (recovery rate = 48%; P = .000 highly significant).
Conclusions:
Vertigo and diabetes mellitus play a negative role in the recovery of SSNHL. The novel treatment protocol we used in group I patients that is liquid glycerol and systemic steroids was significantly better and effective in treating SSNHL as compared to the group II treatment protocol of systemic steroids alone. Hence, we concluded that SSNHL is treatable that too with a good recovery rate.
Introduction
Sudden sensorineural hearing loss (SSNHL) and its management is an unraveled mystery which still needs to be solved. Numerous studies and reviews have been conducted trying to formulate a valid definition and the best management protocol of SSNHL. The most accepted definition of SSNHL is sensorineural hearing loss of 30dB or greater over at least 3 contiguous audiometric frequencies occurring over 72 hours. 1 The management of SSNHL depends upon whether it is idiopathic or of known etiology. Sensorineural hearing loss with known etiology has been postulated to be due to vestibular schwannoma, malignancies, and stroke. 2 In 90% of patients, of SSNHL, cause is not known (idiopathic) and pathogenesis in these patients is attributed to vascular, viral, cochlear membrane rupture, or multiple etiologies. 3
There have been myriad treatment options in the form of systemic and intratympanic steroids, hyperbaric oxygen, carbogen therapy, antiviral and diuretics, and sometimes observation alone. 4 Despite the fact that many studies and American Academy of Otolaryngology—Head and Neck Surgery (AAO-HNS) 4 guidelines of 2012 advocate the use of systemic steroids for the management of SSNHL but still the resultant hearing gain is uncertain and questionable. 5
In the last 2 decades, many researchers have recommended the use of intratympanic steroid therapy in patients with SSNHL as a rescue or salvage therapy and none of the conducted studies could demonstrate superior results in comparison to systemic steroids. 6 -8 So till date an unequivocal answer to this question is still elusive. With this background, we conducted a study, first of its kind, testing the combination of systemic steroid and glycerol in patients presenting with SSNHL.
Systemic steroids in SSNHL have been known to act by their anti-inflammatory properties to improve the clinical outcome. The use of osmotic agent glycerol along with steroids in the management of SSNHL was with the ideology to utilize the osmotic property of this agent in effectively decreasing inner ear fluid pressure. Although the exact etiology of SSNHL is not known but the proposed pathogenesis could be either transudation or exudation of fluid in the inner ear compartment secondary to some vascular or viral insult or cochlear membrane rupture. This transudation/ exudation of fluid leads to raised inner ear fluid pressure and hence causing hearing insult. So we hypothesized that both glycerol and steroids in combination will help in hearing gain by decreasing the inner ear pressure due to osmosis and anti-inflammatory effect, respectively.
We also studied the various parameters known to have prognostic influence on SSNHL such as the age and timing of presentation, associated disorder like diabetes, and symptoms such as vertigo and tinnitus. 9 -11
Materials and Methods
This study was carried out from January 2017 to May 2019 on a total of 150 patients who presented to our ENT and Head & Neck Center. After obtaining an informed written consent from all the patients with SSNHL who participated in the study, they were divided into 2 equal groups on the basis of stratified randomization. Ethical clearance was obtained from the institutional ethical committee, and our study was allotted with the ethical committee number ASCOMS/IEC/2014/107 dated 15-12-2014.
All the patients with idiopathic SSNHL presenting to us within 15 days of first experiencing the symptom of hearing impairment were included in this study.
The patients were further categorized according to their age-groups as follows: age in years <30, 31 to 40, 41 to 50, 51 to 60, and >61 and days of presentation: 0 to 3, 4 to 7, 8 to 11, and 12 to 15 days.
Patients were also divided into early and late presenters. Early presenters were the patients who presented to the our center between 0 and 3 days after experiencing hearing loss and late presenters were the ones who experienced hearing loss between 4 and 15 days. Patients with hearing loss for more than 15 days were excluded from this study. Patients with SSNHL due to known etiologies like infections, any space occupying lesion, Meniere disease, and those younger than 10 years were excluded from our study.
Of the 2 groups consisting of 75 patients in each group, group I (DG) was given a combination of glycerol and steroids for a total of 9 days. The dosing schedule was oral glycerol (1g/kg/d) liquid in 4 divided doses for 9 days and injection dexamethasone 8 mg (weight 50 kg or more) or 4 mg (weight < 50 kg) intramuscularly once daily for first 3 days, followed by oral steroids in the form of tablet deflazacort 30 mg (weight 50 kg or more) or 15 mg (weight < 50 kg) twice a day for next 3 days. Deflazacort was tapered to once daily dosing for another 3 days before discontinuing.
In group II (D), only steroids were administered in the same dosing schedule as in group 1 (DG), that is, injection dexamethasone once daily for 3 days followed by oral tablet deflazacort alone. No glycerol was given in these patients.
Diabetic patients included in the study were managed on the same drug protocol and their blood sugar monitoring was done regularly. Their glycemic status was kept under control using insulin or oral hypoglycemic drug.
At the time of presentation (0 day), in addition to general physical examination, all the 150 patients underwent complete ENT examination including microscopic examination of ear and a battery of hearing tests in the form of pure tone audiogram (PTA), speech audiometry, and impedance audiometry. The hearing tests were repeated at follow-up on third day, 1 week, and third and sixth week.
As a protocol, all patients underwent magnetic resonance imaging brain and relevant blood investigations.
Recovery score for each patient was calculated using the definition of recovery (AAO-HNS), 4 that is improvement to 50% of baseline difference between the treated and untreated ear patients was divided in 2 categories: complete recovery and no recovery. Both the groups were studied for side effects if any.
Based on the above findings, performa for each patient was filled in and analyzed statistically using IBM SPSS software (version 20). The Chi-square test was used for analysis and the power of the study.
Results
The compiled results were compared with respect to hearing gain outcome and the role of various factors such as age, sex, and timing of presentation, associated tinnitus, vertigo, and diabetes mellitus (DM).
Of the total 150 patients with SSNHL, 77 were males and 73 were females and no significant difference was noted in the recovery rates in both the genders and both the groups (group I: P = .13; group II: P = .20).
In group I (DG) and group II (D), the number of patients presenting in different divided age-groups and genders were similar (P = .49 not significant; Table 1).
Patients Divided According to Their Age-Groups and Gender in Group I and Group II.
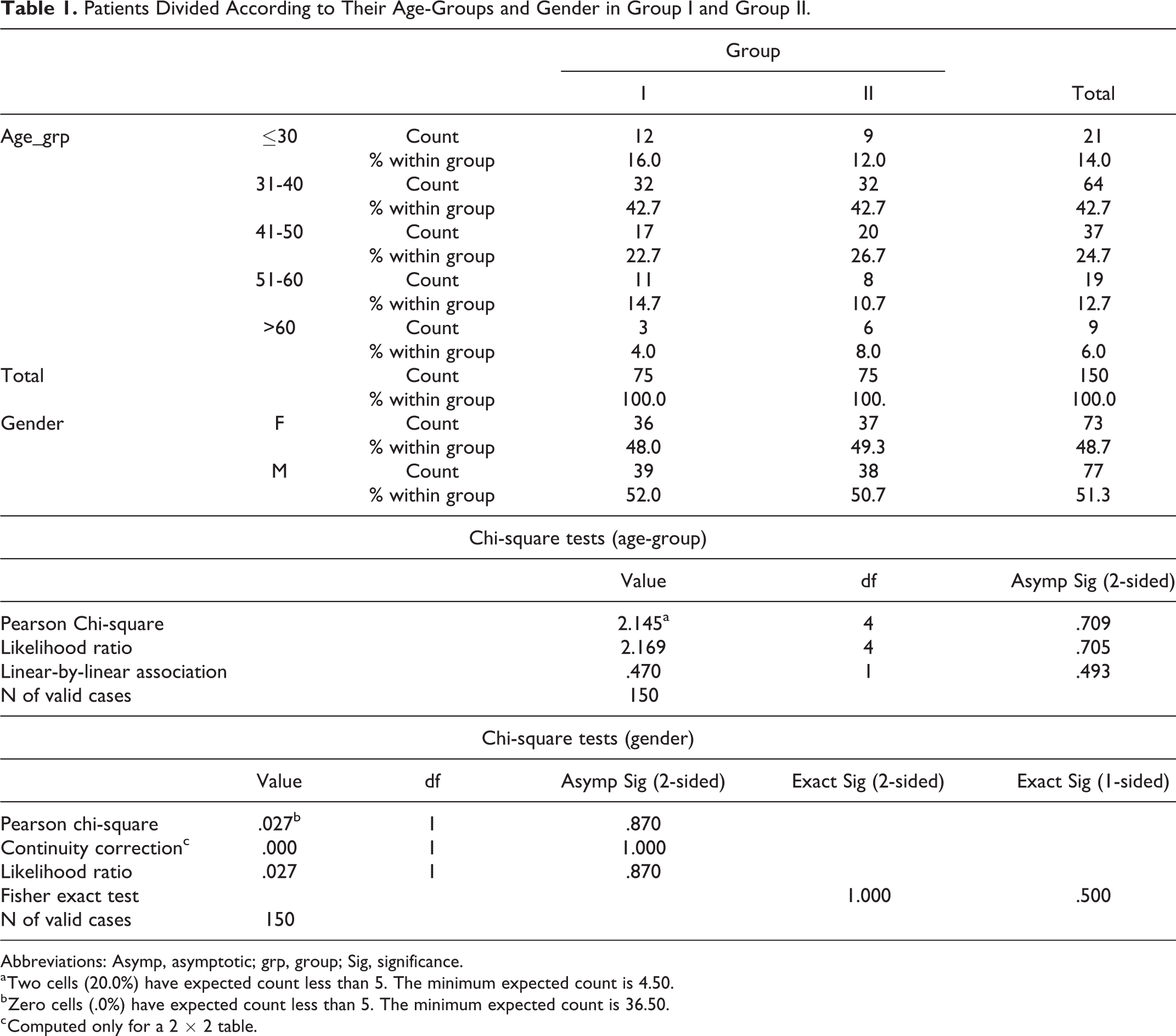
Abbreviations: Asymp, asymptotic; grp, group; Sig, significance.
a Two cells (20.0%) have expected count less than 5. The minimum expected count is 4.50.
b Zero cells (.0%) have expected count less than 5. The minimum expected count is 36.50.
c Computed only for a 2 × 2 table.
The effect of age on the recovery rate was noted. In group I (DG), the recovery pattern in all the divided age-groups was similar (P = .304; Table 2 and Figure 1A).
On the contrary in group II (D), the recovery score of younger patients was much better as compared to the older age-group patients (P < .05 significant; Table 2 and Figure 1B).
Recovery Score in Group I and Group II According to Different Age-Groups.a
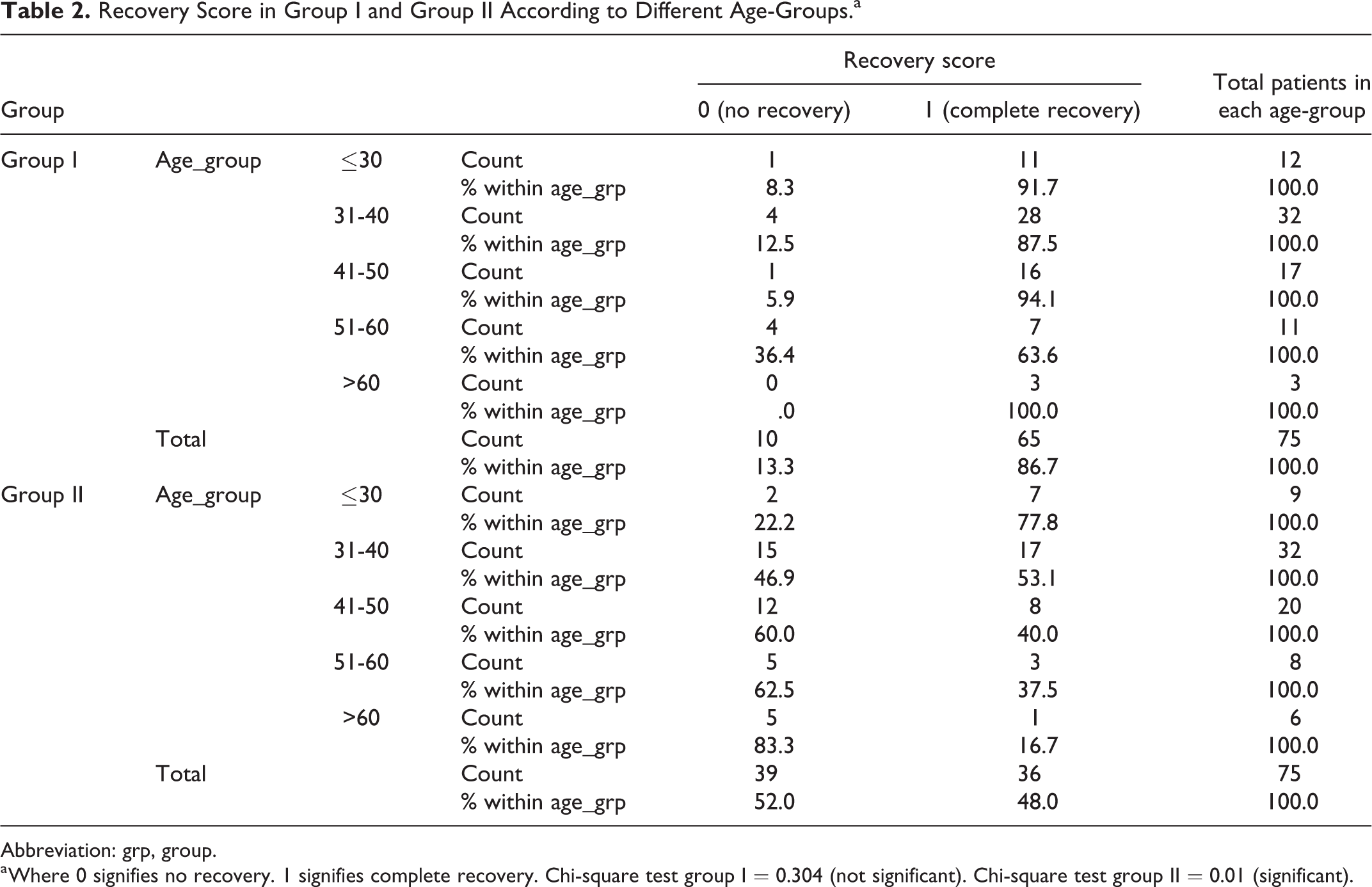
Abbreviation: grp, group.
a Where 0 signifies no recovery. 1 signifies complete recovery. Chi-square test group I = 0.304 (not significant). Chi-square test group II = 0.01 (significant).
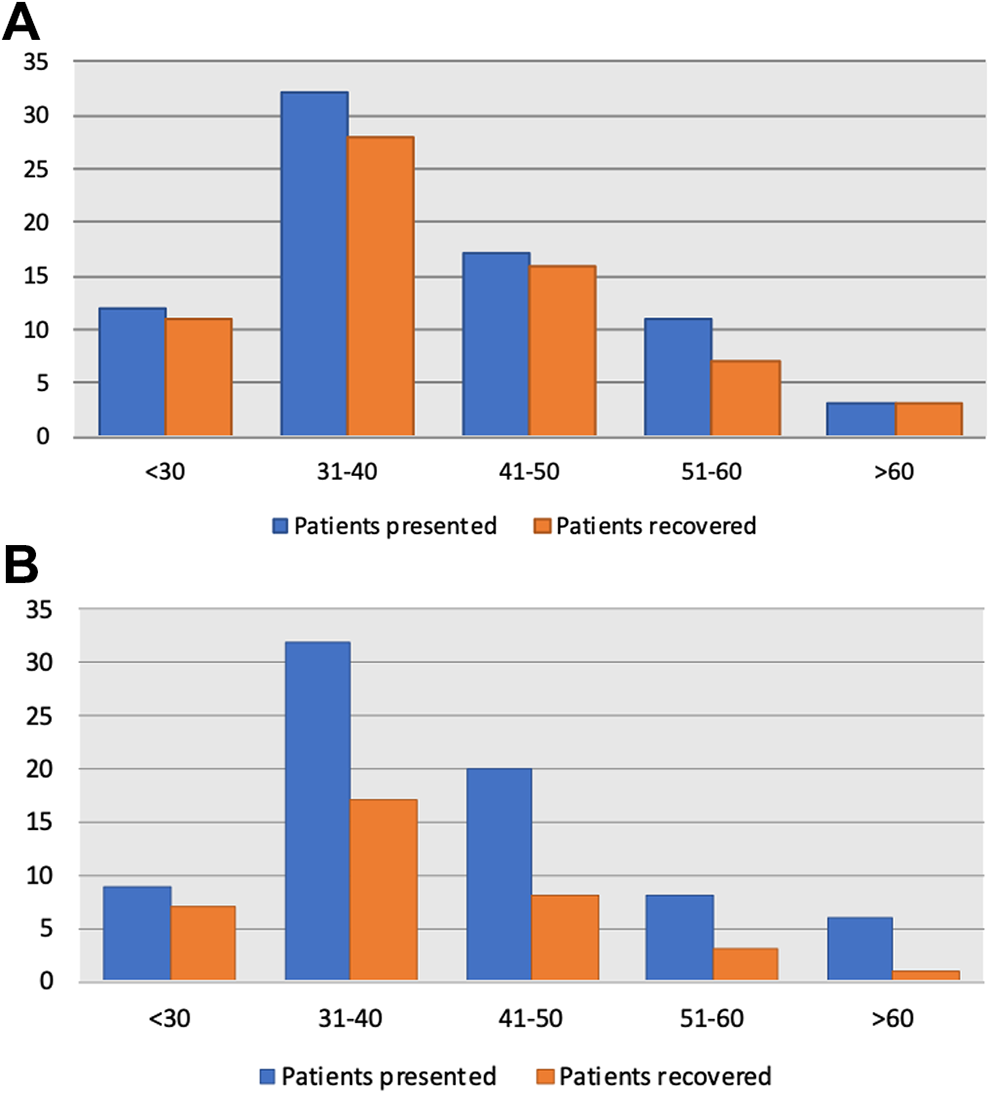
A, Recovery pattern in group I patients in different age-groups. B, Recovery pattern in group II patients in different age-groups.
The relationship of the time of presentation and its effect on the recovery score was noted. In group I (DG), we found that there was no significant difference in recovery of patients presenting early or late (P > .05). On the contrary in group II (D), a significant impact of days of presentation on the recovery score was found; wherein early presenters (hearing loss < 3 days) showing better recovery as compared to late presenters (hearing loss > 3 days; P < .001; Table 3; Figure 2A and B).
Recovery Score in Group I and Group II According to the Days of Presentation.a
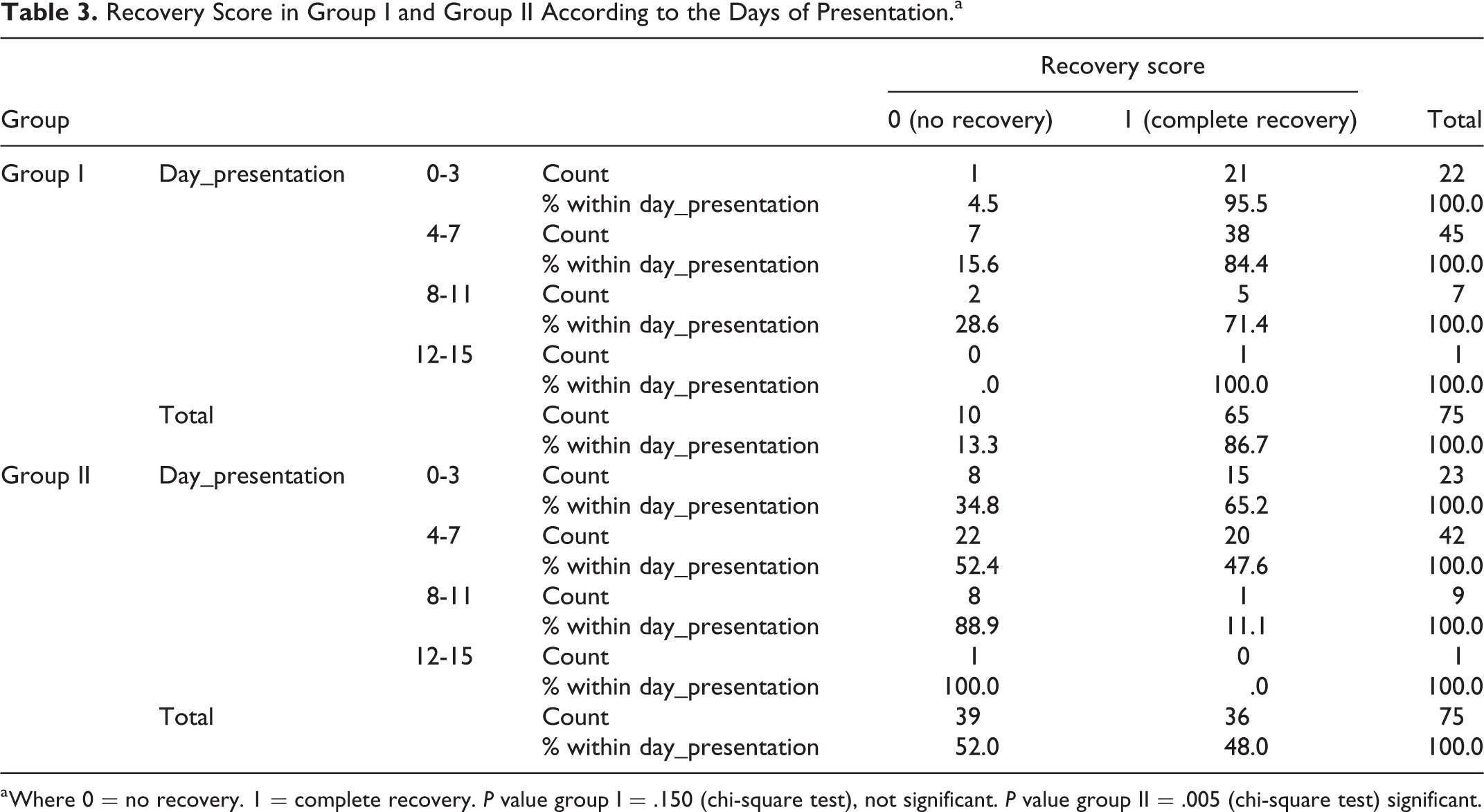
a Where 0 = no recovery. 1 = complete recovery. P value group I = .150 (chi-square test), not significant. P value group II = .005 (chi-square test) significant.
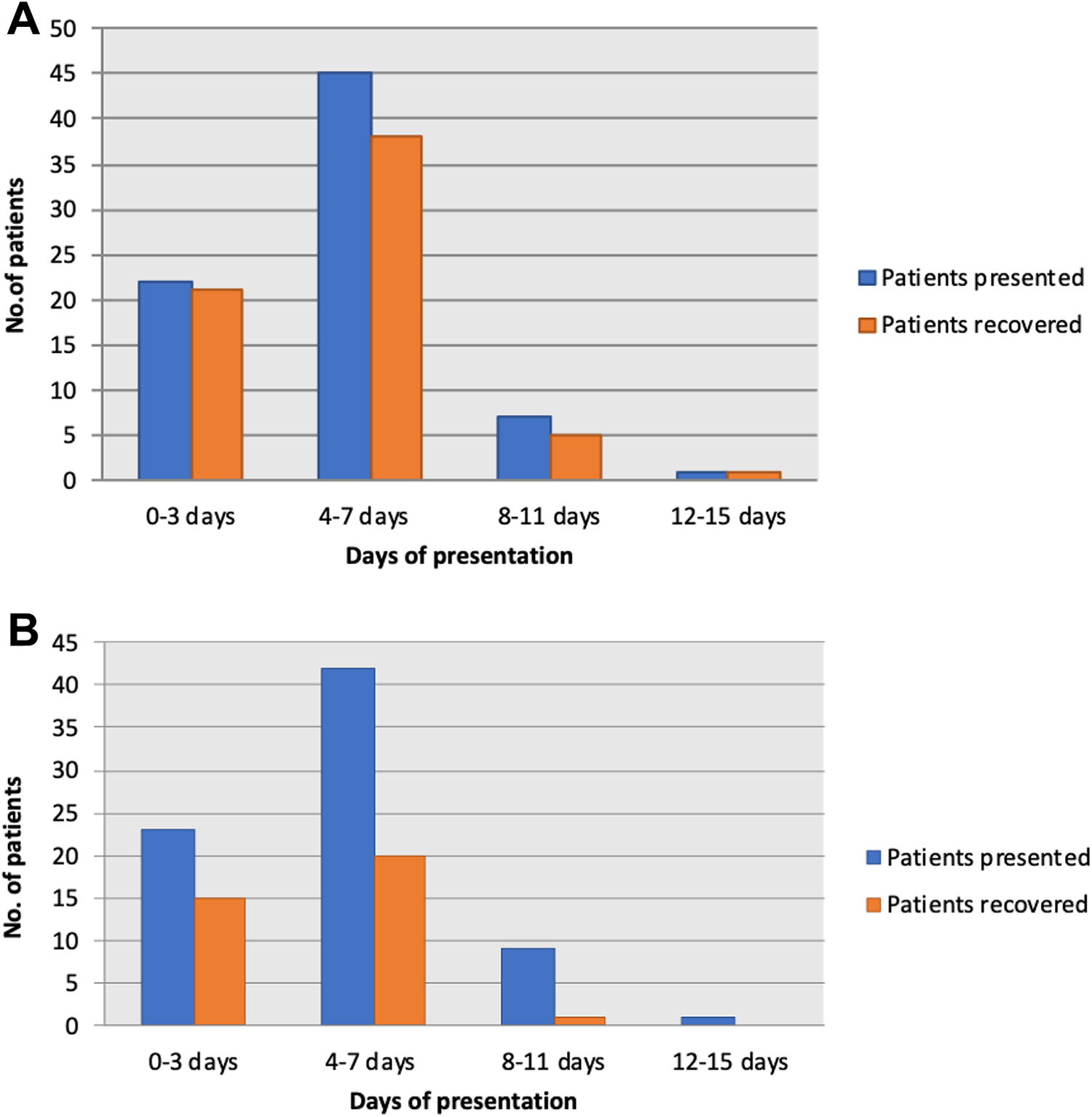
A, Recovery pattern in group I according to the days of presentation. B, Recovery pattern in group II according to the days of presentation.
Of 150 patients, 19 were known diabetics, and recovery rate was poor in all these patients. In group I (DG), there were a total of 12 patients who had diabetes and only 6 patients recovered thus showing a poor response to treatment (P < .001 highly significant). In group II (D), a total of 7 patients were diabetics and none recovered (P < .001 highly sig).
Another factor analyzed in relation to its impact on recovery rate on SSNHL was the presence of vertigo and tinnitus.
Patients presenting with vertigo as an accompanying symptom with SSNHL had a poor recovery rate. In group I (DG), a total of 4 patients experienced vertigo and none recovered from SSNHL (P < .001 highly significant).
In group II (D), a total of 6 patients experienced vertigo and none of them recovered too (P < .001 highly significant).
Tinnitus on the other hand did not show any significant impact on the recovery rate of patients with SSNHL (group I P = .15 not significant, group II P = .12).
The mean PTA score on day of presentation (day 0) and at the end of 6 weeks was also compared in both the groups. In group I (DG), the mean PTA values at day of presentation was 61.40 and at the end of 6 weeks was 30.31 (P value < .001 highly significant). In group II (D), mean PTA values at the day of presentation was 61.36 and at the end of 6 weeks was 43.05 (Table 4).
Mean PTA Improvement at Day 0 and at Sixth Week in Group I and Group II.a
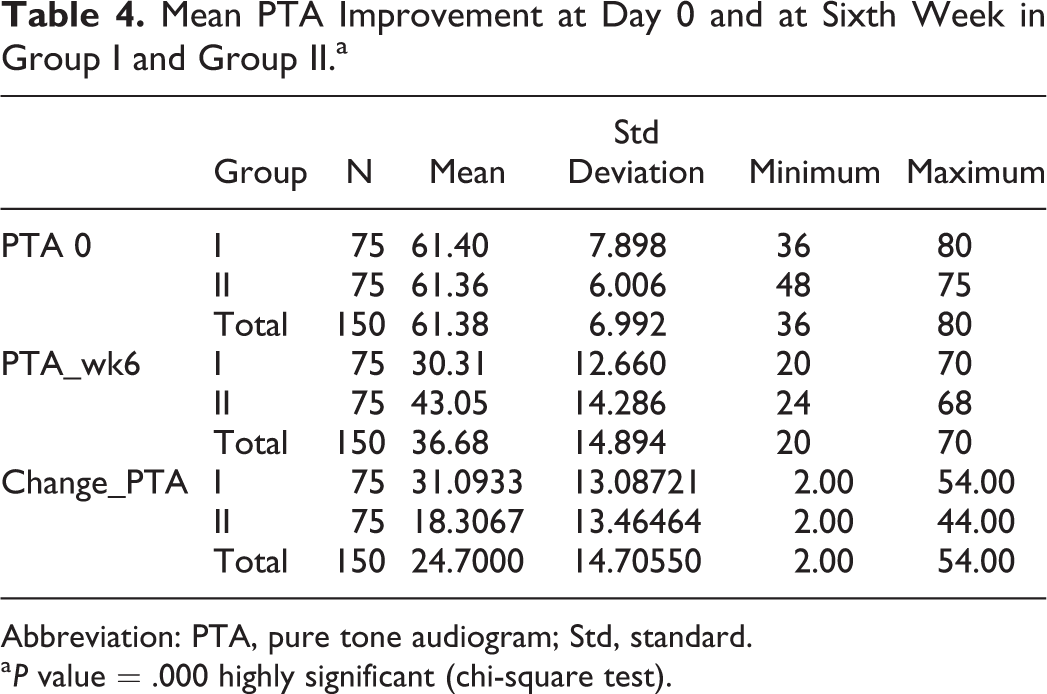
Abbreviation: PTA, pure tone audiogram; Std, standard.
a P value = .000 highly significant (chi-square test).
Finally the comparison of recovery rates in group I (glycerol + steroid) and group II (steroid alone) showed a significantly higher recovery rate (86.7%) in group I as compared to group II (48%; P < .001; Table 5 and Figure 3).
No untoward incident was reported by any of the patients in both the groups.
Comparison of Recovery Score in Group I and Group II.a
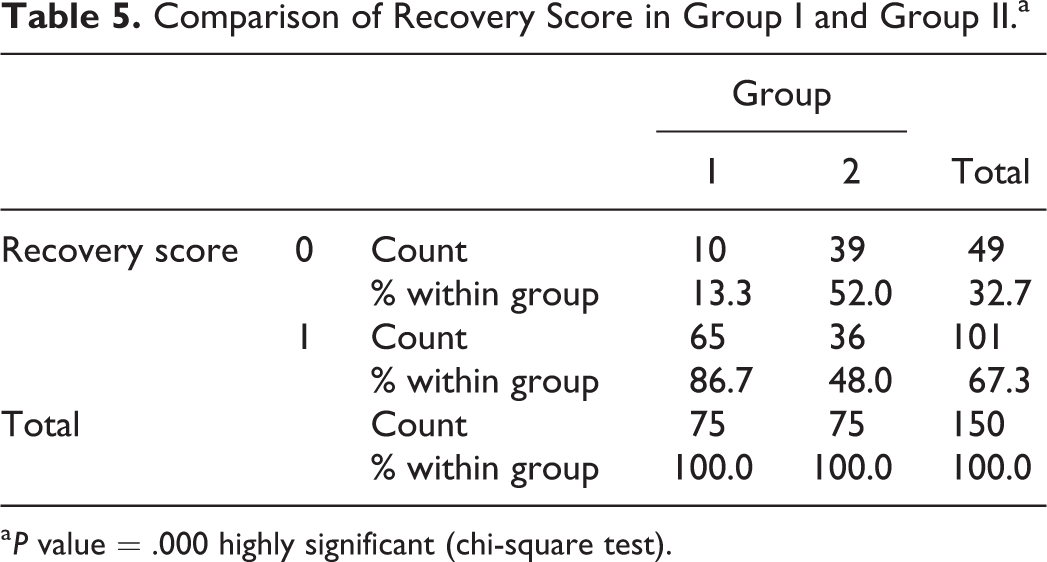
a P value = .000 highly significant (chi-square test).
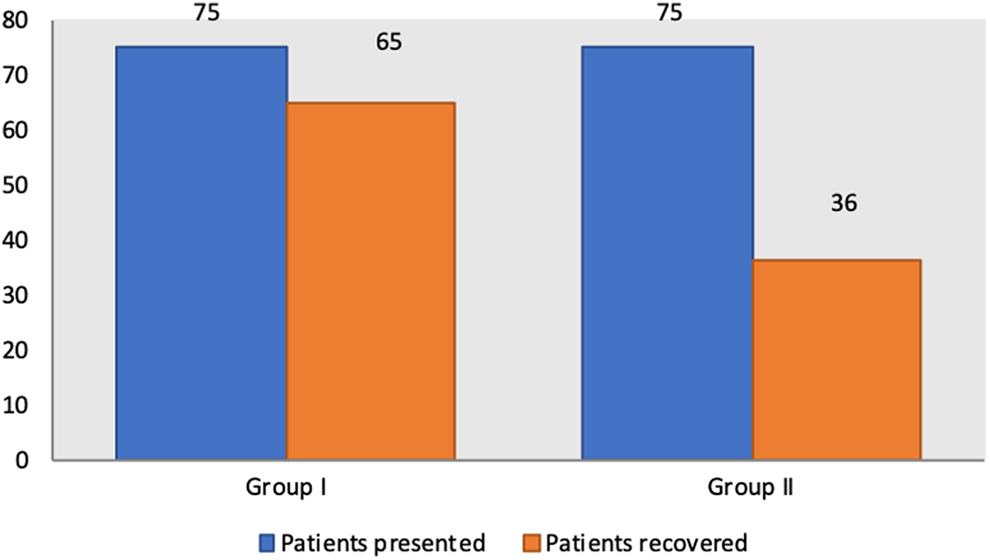
Recovery score in group I and group II.
Discussion
A plethora of studies have been conducted in past testing various modalities of treatment like intratympanic steroids, hyperbaric oxygen, and magnesium, however every study had its own limitation. 4
Traditionally systemic steroids have been tried alone yet the desired outcomes have not been achieved with their administration.
Many authors have advocated the use of intratympanic steroids and various treatment regimens, ranging from its use as primary therapy, adjuvant therapy with systemic steroids, or as rescue or salvage has been studied. The outcome of intratympanic steroids is similar to use of systemic steroids alone without much additional benefits. Also patients are more comfortable with less invasive techniques. 6 -8
This study was an endeavor to find an effective management of SSNHL and also to identify various factors which influence the outcome of treatment.
A novel combination of drugs glycerol and systemic steroids was given for 9 days, which to our knowledge has not been used previously for this purpose. Glycerol, an osmotic agent, was added in addition to steroids with the ideology that it is a well-known drug which reduces the inner ear pressure. Hearing recovery was seen in relation to various parameters like age, timing of presentation, and diabetes. Associated symptoms of vertigo and tinnitus were also studied as they are known to have prognostic influence on SSNHL.
Although age is an important factor that has a bearing on hearing recovery and in many studies advancing age (>60 years) has been universally correlated with decrease rates of hearing recovery and lower absolute threshold gains. 5,9 Interestingly, in patients of group I where glycerol was added, the patients of all age-groups whether young or old had significantly good recovery; whereas in group II (D) patients, we noticed that with the increasing age there was a decreasing trend in the recovery rate (Table 2; Figure 1A and B). So patients of advancing age can benefit from the administration of glycerol along with steroids in case of SSNHL.
Timing of presentation that is the delay in seeking medical advice is another prognostic factor influencing the course of SSNHL recovery. 9 -11
Early presentation of patients especially less than a week after onset of SSNHL correlates with improved odds of hearing recovery. 12
In the present study, the cutoff point of patients presenting with hearing loss was 15 days, so no patient presenting with the complaint of SSNHL beyond the above mentioned time span was included.
The decision to take this time frame was based upon the evidence found in literature which clearly indicated the best time to act upon SSNHL is first 2 weeks and instituting treatment beyond this would outweigh the risk-to-benefit ratio.
Early presentation to a physician (less than a week) after onset of SSNHL correlates with improved odds of hearing, with chances of complete hearing recovery decreasing after that time. 13 -17
In the present study surprisingly both early and late presenters, who received glycerol in addition to steroids, had a notably good hearing gain (Table 3 and Figure 2A) Results of our study show a definitive role of oral glycerol for better outcome in patients with SNHL irrespective of age and time of presentation. The possible explanation of role of glycerol in addition to steroids in hearing improvement could be attributed to the anti-inflammatory action of steroids on hair cells and dehydrating action of glycerol on inner ear pressure. This effect of glycerol and systemic steroids on cochlea could be the reason to explain the improvement in hearing even in old age patients and late presenters.
Diabetes is one of the systemic disorders known to be associated with SSNHL, and the previous studies show that recovery is not good with any of the treatment modalities. Min-Beom Kim et al studied the effect of diabetes on sensorineural hearing loss and found that the rate of hearing loss in participants with normal glucose levels, prediabetes, and DM was 1.8, 3.1, and 9.2, respectively, per 1000 person-years and concluded that patients with DM having a moderately increased risk of future hearing loss 18 . In the present study the number of diabetics included were limited as there were 12 diabetic patients in Group I and 7 in Group II. The hearing gain in diabetic patients was insignificant, it was observed that only 6 patients in glycerol plus steroid (Group I) none in streoid group (Group II) had any recovery.
This could be explained by the fact that DM is a metabolic disorder affecting all the systems of body by way of progressive microangiopathies resulting in impaired microcirculation. From the knowledge of anatomy of inner ear, we know that its blood supply is from the end arteries without any collateral circulation. Hence in diabetic patients due to impaired circulation, the damage to the inner ear will be more and chances of recovery will be poor once there is concurrent SSNHL. As the incidence of diabetes is increasing globally, so a lot of emphasis should be laid on good glycemic control.
An association of vertigo and tinnitus is very commonly seen with SSNHL. Many studies have analyzed the correlation between these symptoms on the course and recovery of SSNHL.
Interestingly, a negative impact of vertigo on SSNHL was found in this study. This could possibly be explained by the fact that majority of times vertigo occurs due to disease in vestibular part of the inner ear. The involvement of both the parts of inner ear that is vestibular and cochlea in cases having associated vertigo with SSNHL has poor outcome as compared to involvement of only cochlea in SSNHL without vertigo. Similar results were reported by a study conducted by Moskowitz et al who reported the association of vertigo with SSNHL with poor prognosis as they noticed that only 14% of patients with vertigo achieved a complete recovery. 19 Many studies have not found any correlation between vertigo and SSNHL. 10,12,16,17
Tinnitus as an accompanying symptom of SSNHL has variable reviews, some authors found it to be a positive prognostic factor, 20 others as a negative prognostic factor, 21 and many of them found its presence to be insignificant in patients with SSNHL. 10,14 A study conducted by Nosarti-Zarenoe et al 14 found that the presence of tinnitus as an accompanying symptom did not show any significant influence on hearing recovery score which was similar to the results of our study, where no effect of tinnitus on hearing recovery was seen in both the groups.
The mean pure tone audiometry score difference (showing improvement) on the day of presentation and at sixth week of analysis was 31 dB in glycerol plus steroid group versus 18.3 dB in steroid group showing a marked PTA improvement in group I patients at the end of sixth week (Table 4).
A comparison of hearing recovery scores showed 86.5% recovery in patients receiving glycerol in combination with steroids and only 48.2% recovery in patients receiving steroid alone (P < .001 highly significant; Table 5 and Figure 3).
So, according to this study glycerol and steroid are the answer in patients with SSNHL to achieve a good hearing recovery. The limitation of our study is the small sample size which was calculated on the basis of statistical analysis of a pilot feasibility study conducted on 40 patients in our center.
Conclusion
The treatment protocol using combination of glycerol and steroids in the management of SSNHL gives better results as compared to steroids alone. There were a few factors such as DM and vertigo which are associated with lower recovery of SSNHL. The overall outcome and recovery were significantly better in patients with SSNHL who received glycerol in addition to steroid irrespective of the age-group and timing of presentation. Hence glycerol in addition to steroids has a definitive role in the management of patients with SSNHL, and this combination benefits all age-groups of patients and even effective in late presenters up to 2 weeks.
With years of research work and arrays of treatment protocols being designed aiming to reduce the occurrence of permanent disability caused by SSNHL, the present study was able to achieve the desired goal to some extent. However, a larger number of patients with specific conditions like DM, tinnitus, and vertigo and so on need to be studied and late presenters presenting beyond 2 weeks need to be taken up in order to reach a definitive conclusion of outcome and their management.
Hence a larger multicenter study is required to support the use of glycerol in addition to steroids as a standard of treatment in patients with sudden onset sensorineural hearing loss.
Footnotes
Acknowledgments
This article and the research would not have been possible without the exceptional support of my mother, Nandita Mehta, who is an anaesthesiologist and a very good editor as well. Her enthusiasm, knowledge, and exacting attention to detail have been an inspiration and kept my work on track from my first draft to the final draft of this article. I would also like to extend my thanks to Mr Vipin Kumar, audiologist at our center, who has helped me with all the audiometric evaluations of my patients and without his support managing the performa’s of so many patients wouldn’t have been possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.