
Abstract

A 28-year-old otherwise healthy female presented with right-sided hearing impairment for 1 year, and tinnitus exacerbation in recent 1 month. Physical examination revealed no neurological deficits. Pure tone audiometry revealed a mild sensorineural hearing impairment with an average of 36 dB and a speech discrimination score of 30% in the right-sided ear. The patient underwent magnetic resonance imaging (MRI), which revealed an enhancing mass measuring 9 mm × 18 mm at right internal auditory canal (IAC), and was laterally extending without fundal fluid (Figure 1). The patient was diagnosed as vestibular schwannoma (VS) and received Gamma Knife (GK) with a tumor margin dose of 13 Gy. However, 5 days following treatment, the patient developed acute facial palsy with House-Brackmann Grade V. She received systemic steroid treatment for 1 month. Unfortunately, her hearing loss and House-Brackmann Grade IV persisted after 1-year follow-up.
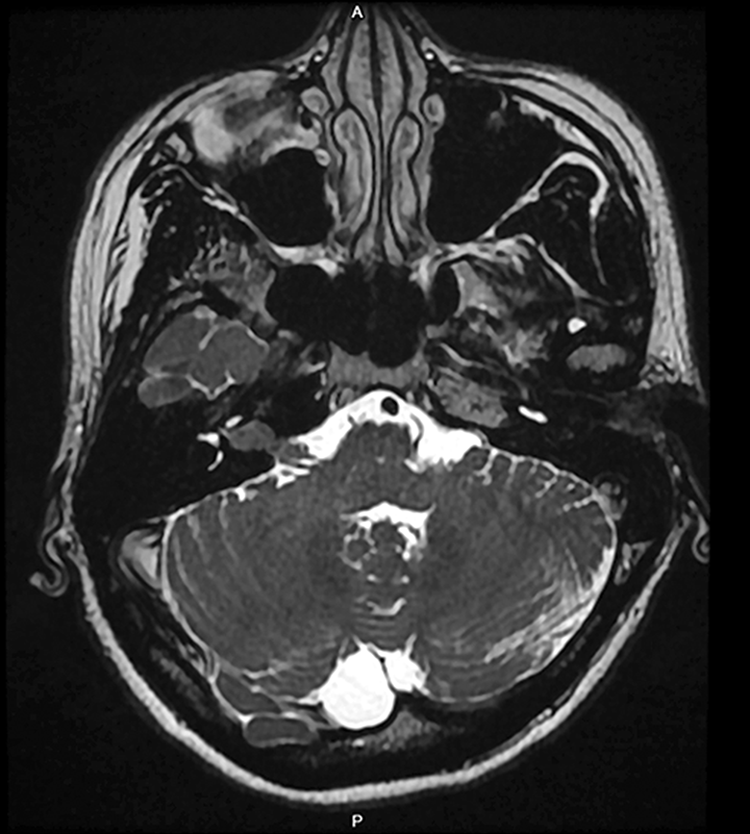
An enhancing mass measuring 9 mm × 18 mm at the right internal auditory canal, causing expansion of the canal, and was laterally extending without fundal fluid collection.
Stereotactic radiosurgery (SRS) is now widely used and multiple studies have demonstrated the general safety and efficacy, and there will be an increase in the number of SRS-managed patients with VS. 1 Hence, it is more important to study specific complications and its risk factors following SRS. Lerner et al pointed out 71% of subjects who developed facial paresis after GK had tumors that were laterally positioned and lacked fundal fluid on preoperative MRI imaging. 2 Interestingly, our presented case had similar radiographic characteristics with their report.
The “fundal fluid cap,” also known as cerebrospinal fluid in the IAC on MRI imaging, which presence may be associated with tumor size, emerged as a variable and thus became an area of interest in VS.3,4 Lerner et al found that tumors without fundal fluid on MRI imaging experienced higher rates of facial paresis after GK treatment. 2 However, conflicting evidence of a radiographic fundal fluid cap has noted from recent studies through surgical approaches. 5 Sullivan et al documented larger fundal fluid caps trended toward worse postoperative facial nerve outcomes. 6 Sun et al concluded that radiographic presence of fundal fluid or its size was not significantly correlated to hearing outcome. 5 These observations call into question the prognostic value of a fundal fluid cap, and require further corroboration in a larger study population.
We emphasize that VS tumors that were laterally positioned and lacked fundal fluid on imaging trended toward the complication of facial nerve paresis after GK concomitant with a poor outcome of recovery, and the radiographic fundal fluid cap may be taken into account during making management decisions for patients with VS.
Footnotes
Authors’ Note
The patient’s identity is not identifiable through the figures and research information, patient consent statement is not added.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-D-109053 to H.-C. Chen).