
Abstract
Introduction:
Despite good results of transoral laser CO2 microsurgery (CO2TOLMS) of the larynx, a lack of data related to the safety of this technique as a day-case procedure across the literature is evident.
Materials and Methods:
An observational, retrospective, non-randomized study.
Results:
One hundred four (62.6%) patients met the inclusion criteria, 96 (92.3%) patients were male, and 8 (7.7%) patients were female. The mean age of the study group was 66 ± 11 years (min: 34/max: 90). All the patients underwent CO2TOLMS were treated as an outpatient procedure. The glottis was the most common location affecting 97 (93.3%) patients, regarding the need of readmission, just 4 (3.8%) patients needed to be readmitted after surgery due to dyspnea secondary to laryngeal edema in 2 cases by laryngeal bleeding, and cervical emphysema in one case, respectively. Being just necessary to reintubate 1 patient (<1%) to control the bleeding. We didn’t find any statistical correlation between variables and the need for readmission of reintubation.
Conclusion:
According to our results, CO2TOLMS of the larynx can be safely performed as an outpatient procedure. To establish a proper protocol and to perform a careful preoperative assessment are essential to increase our success rate and to prevent any potential complication.
Introduction
Transoral laser CO2 microsurgery (CO2TOLMS) of the larynx is a well-established surgical technique that has gained followers around the world during the last 4 decades, becoming the gold standard for almost all premalignant lesion (Dysplasia, leucoplakia, etc) and malignant early-stage cancer (Tis-T2). It also represents a safe and useful technique, associated with excellent locoregional control, overall survival, and disease-free survival, comparing with other methods. 1 -6
Despite the extended use of this technique and the feasibility as a day-case procedure, there is a lack of studies analyzing the risk and the rate of readmission when it is used in such a way. In spite of this, the present study aims to describe the safety of CO2TOLMS as an outpatient procedure in a group of patients treated for malignant and premalignant lesions of the larynx in a tertiary university hospital.
Material and Methods
After the approval of the ethics committee of our institution, a retrospective analysis of data prospectively collected from 104 patients diagnosed with a larynx lesion and treated with CO2 TOLMS between July 2016 and July 2018 was performed. Those patients with definitive malignant histology were staged according to the criteria of the Union Internationale Contre le Cancer and the American Joint Committee on Cancer.
Demographic data, medical background, tumor stage in case of malignancy, diagnostic tests information, final histology, definitive size of the tumor reported by the pathologist, type of surgery, surgical complications, the need to visit the emergency room, and the need to be readmitted at the hospital were collected in the head and neck database of our department by the main author. Visits at the emergency room or need of readmission associated with exacerbation of chronic diseases that were not possible to associate to the use of this technique were excluded.
To consider a patient as a candidate for an outpatient CO2 TOLMS of the larynx, a careful examination was performed in the clinic, taking into account comorbidities, familiar support, tumor or lesion characteristics, laryngeal structures affected and anatomical conformation of the mouth and neck of the patient. Those criteria followed in our department to elect candidates for an outpatient procedure were described in Table 1. General anesthesia with orotracheal intubation with special tubes for laser surgery (Laser-Shield II; Medtronics, and Mallinckrodt; Covidien) was used. During the procedure, the O2 level was reduced, and the cuffed tube was protected in its proximal portion with cotton sponges moistened with saline. To expose the larynx, we use a Weerda laryngoscope or Kleinsasser laryngoscope (B, C, or D) according to the type of lesions. The resection was performed using a Smartxide 2 Laser Co2 device (Deka), with a power setting of 2 to 6 W, used in superpulsed mode and continuous setting, varying size and shape of the spot according to the moment of the surgery using the micromanipulator. The type of resection was classified according to the European Laryngological Society (ELSOC) proposal for glottic 7,8 and supraglottic endoscopic resections. 9 Technique report was done according to the consensus nomenclature of ELSOC. 10 In the case of small tumors (T1a, T1b), whenever possible, en bloc resection was attempted, and after resection, the piece was pinned and oriented in a corkboard.
General Patient Selection Criteria for Day-Case Procedures at Donostia University Hospital.
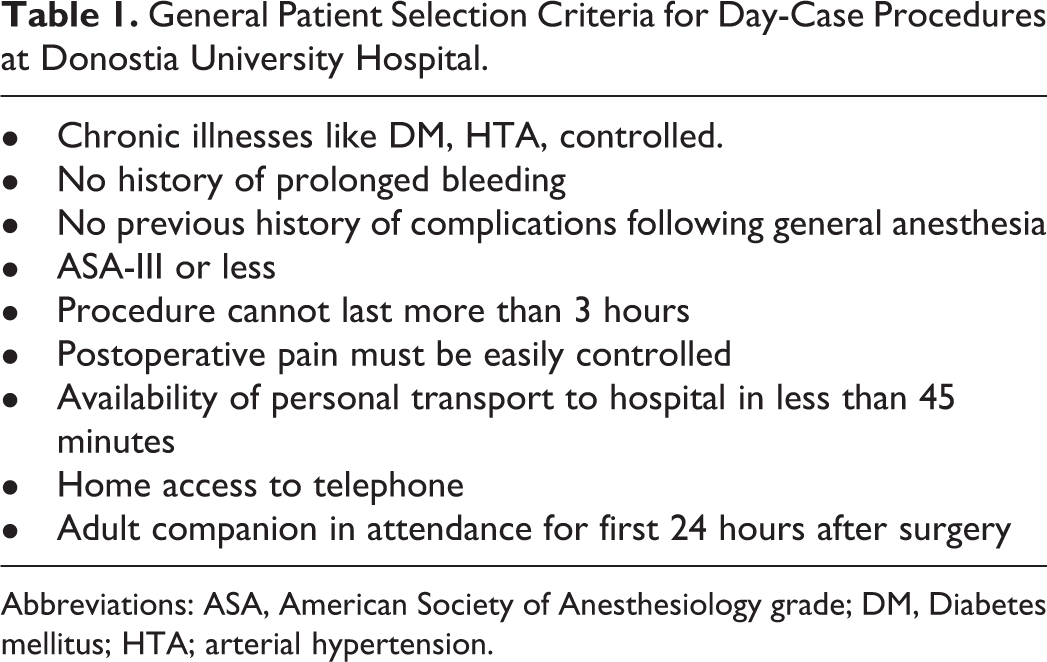
Abbreviations: ASA, American Society of Anesthesiology grade; DM, Diabetes mellitus; HTA; arterial hypertension.
Laser vestibulectomy was performed when a ventricular fold hid the lateral or anterior portion of a tumor. And surgeons tried to achieve a margin of healthy tissue of 1 to 3 mm, attempting to preserve function without affecting the oncological radicality of the procedure when it was necessary.
In all cases, 1 mg/kg of intravenous methylprednisolone was administrated at the onset of intubation, and all patients remained for 2 hours in the postanesthetic recovery room. Patients then remained in the hospital at least 6 hours. During this period, they received a standardized postoperative treatment that included analgesics together with a further dose of 0.5 to 1 mg/kg of methylprednisolone 5 to 7 hours after extubation. The discharge was usually after review by an ENT registrar or a training nurse. All patients were required to eat, urinate, walk, and to be pain-free before discharge.
Statistical analysis was performed using SPSS for Windows, version 21.0 (SPSS, Inc). Quantitative variables in the study were expressed as mean ± SD. The potential associations between epidemiological or clinical variables and outpatient CO2TOLMS of the larynx outcome were assessed through cross-tab generation between 2 variables (binary or categorical variables) and χ2 test. Students t test was used for unpaired data. A P value <.05 was considered significative.
Results
One hundred thirteen patients met the inclusion criteria, from those 104 (92%) were included in the final analysis, while 9 (8%) patients were excluded because of the need to remained hospitalized at least for 24 hours for different reasons (Table 2). Ninety-six (92.3%) patients were male, and 8 (7.7%) patients were female. The mean age of the study group was 66 ± 11 years (min: 34/max: 90). Twenty (19.2%) of these were diabetic, 59 (56.7%) were hypertensive, 67 (64.4%) were smokers, and 44 (42.3%) consumed alcoholic beverages. All the patients underwent CO2TOLMS were treated as an outpatient procedure. The glottis was the most common location affecting 97 (93.3%) patients. The rest of the demographic variables are described in Table 3.
Cause to Remain Hospitalized After CO2TOLMS.
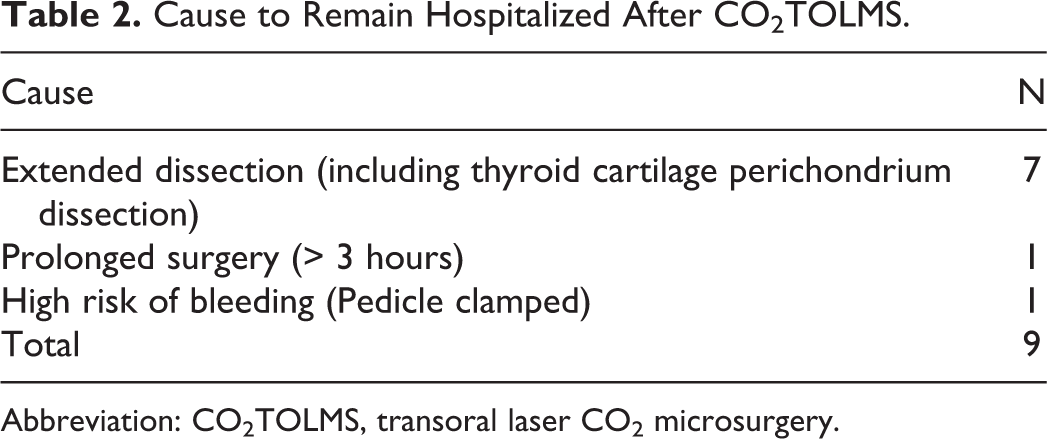
Abbreviation: CO2TOLMS, transoral laser CO2 microsurgery.
Demographic Data of Patients Included.
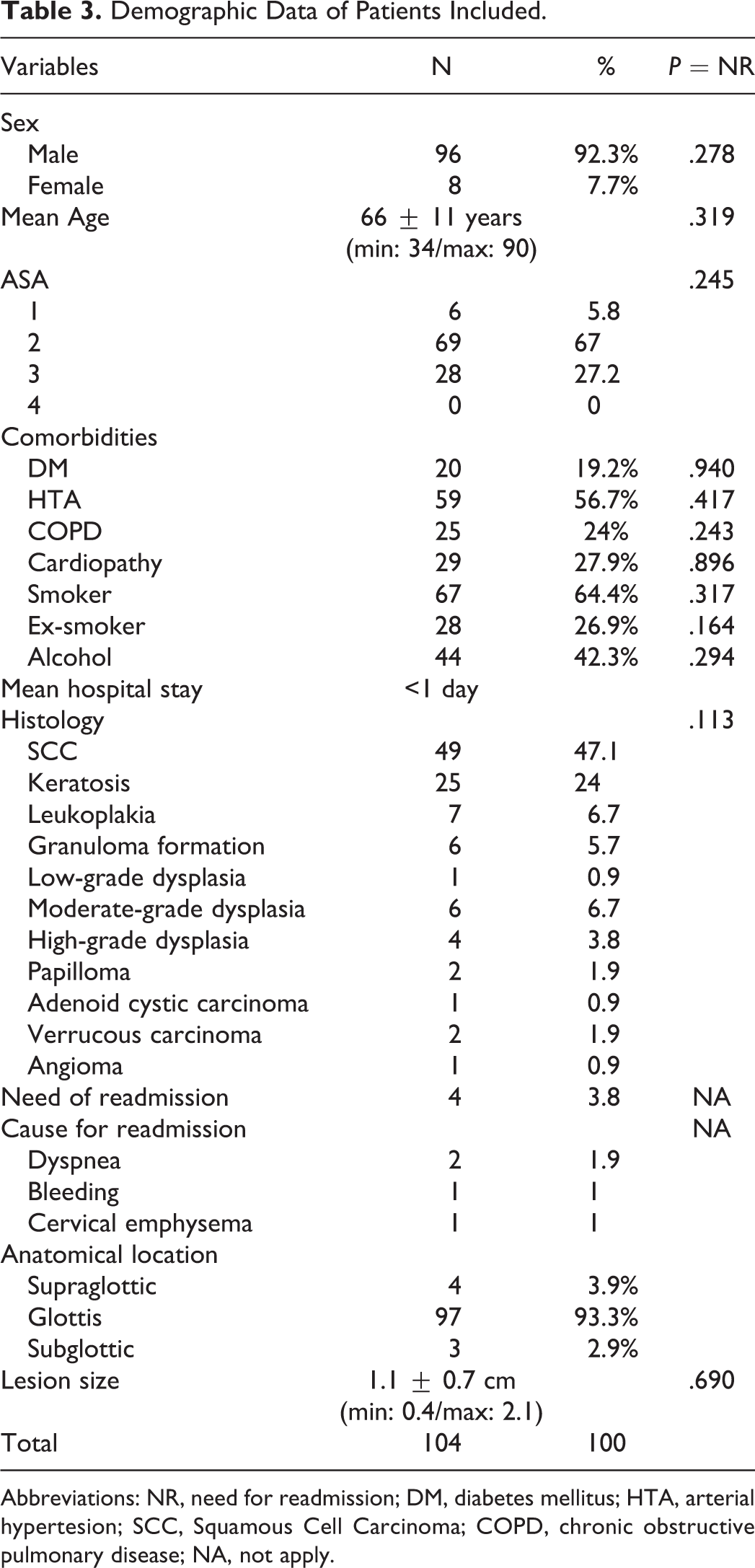
Abbreviations: NR, need for readmission; DM, diabetes mellitus; HTA, arterial hypertesion; SCC, Squamous Cell Carcinoma; COPD, chronic obstructive pulmonary disease; NA, not apply.
Regarding the need for readmission, just 4 (3.8%) patients required to be readmitted after surgery. The cause for readmission was dyspnea secondary to laryngeal edema in 2 cases, laryngeal bleeding and cervical emphysema in 1 case, respectively. Being just necessary to reintubate one patient (1%) to control the bleeding. We didn’t find any statistical correlation between variables and the need for readmission or reintubation.
Data about the type of cordectomy is presented in Table 2: in glottic tumors type I was the most common type, performed in 40 patients, while for supraglottic tumors, the type IIIa was the most common one, performed in 3 patients. However, 19 (14.8%) resection couldn’t be classified. There was no correlation between the type of cordectomy and the need for readmission or reintubation (P = .269; Table 4).
Type of Cordectomy.
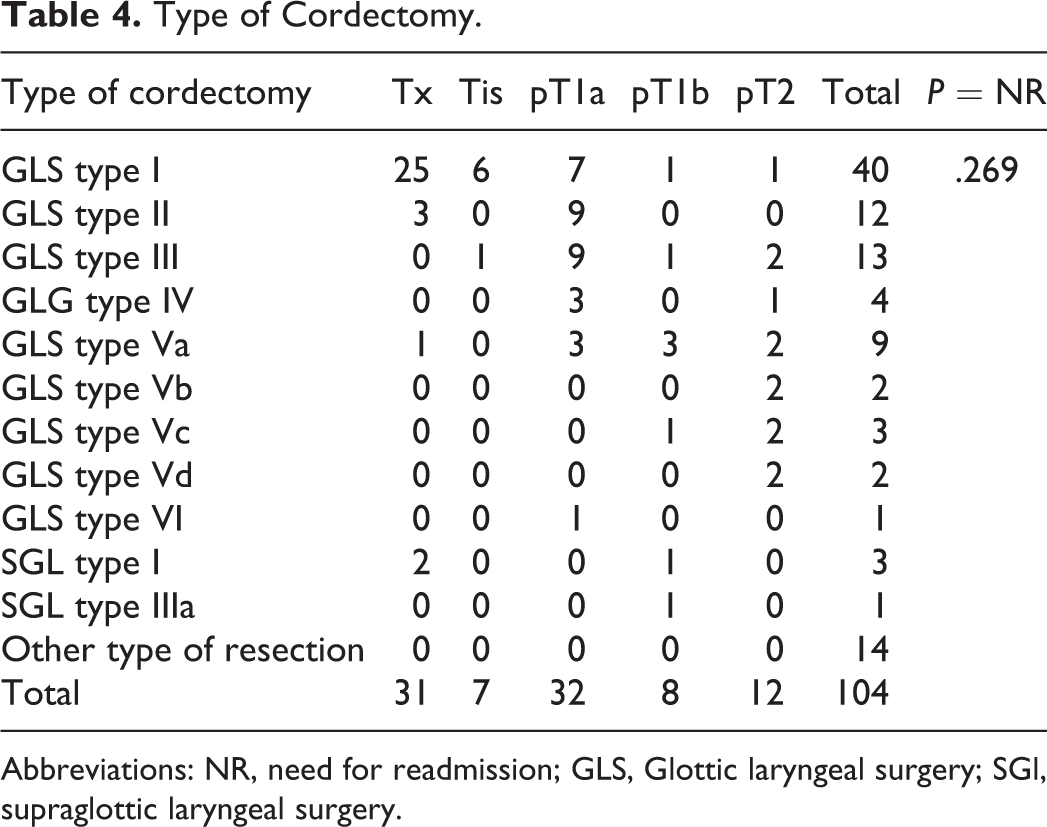
Abbreviations: NR, need for readmission; GLS, Glottic laryngeal surgery; SGl, supraglottic laryngeal surgery.
The rate of perioperative complications was 10.6% (11/104), and in 7 patients, this corresponds to a minor complication and in 4 cases a major complication (P = .492). The type of complications is described in Table 5.
Perioperative Minor and Major Complications in CO2TOLMS. Including Intraoperative and Postoperative Complications.
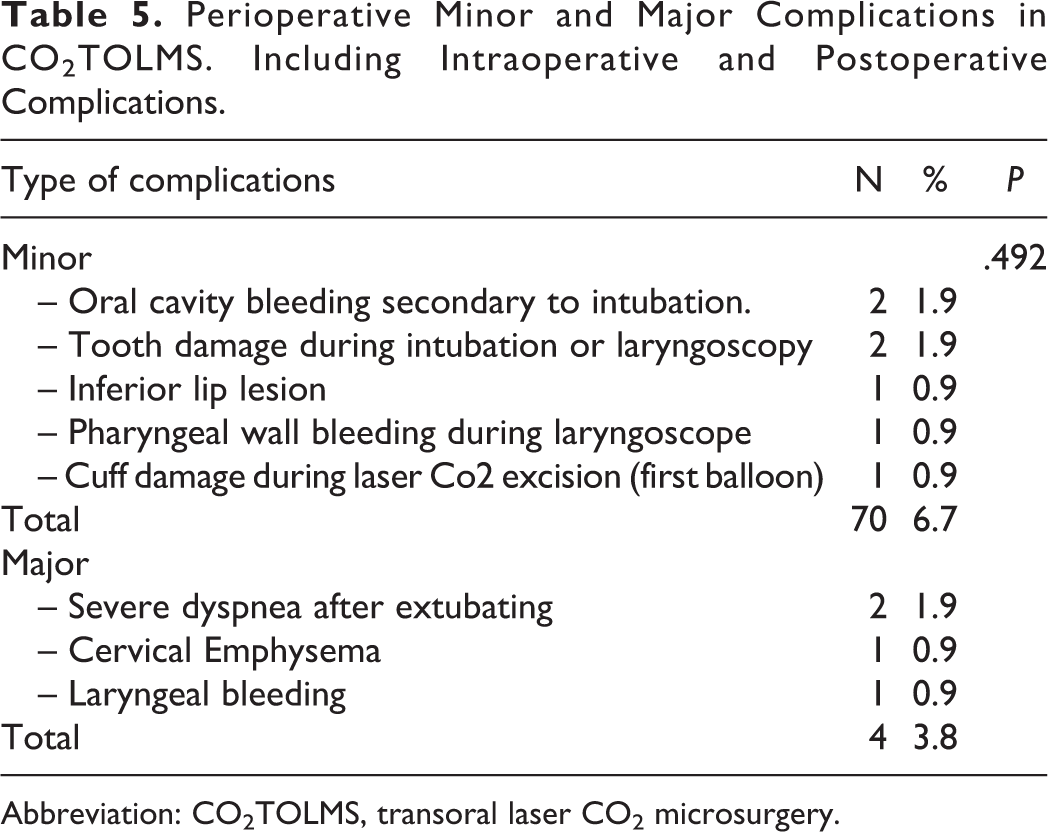
Abbreviation: CO2TOLMS, transoral laser CO2 microsurgery.
Discussion
During the study period, 104 (62.6%) of cases that were treated by CO2TOLMS were scheduled for an outpatient procedure, according to clinical and epidemiological criteria. From these, just 4 cases (3.8%) needed to be readmitted, without significant consequences for the patient in any case. Also, we were not able to find any statistical correlation between comorbidities, histology, size of the lesion or type of comorbidities, and the need of readmission. Results that might be related to the small number of patients who required to be readmitted, a fact that support selection criteria established in our department.
As other authors highlighted before, Co2TOLMS represents a highly efficient technique to treat malignant or premalignant lesion of the larynx that allows patients to come back to their normal life quickly. Moreover, in comparison with other techniques, like the classical open laryngeal approach for early-stage tumor, or with organ preservation techniques like radiotherapy, Co2TOLMS represents a cost-effective method due to the decrease in the need for hospital admission, sick leave, transportation expenses, and functional sequelae.
The safety of outpatient direct laryngoscopy has been challenged in the literature owing to the fear of postoperative airway compromise. However, according to our results and the previous data published, defining rigorous inclusion criteria and following some recommendations described previous reports like the use of postoperative steroids and postoperative surveillance at least 2 hours after surgery in the recovery room, 11,12 those risks related to the airway manipulation can be significantly reduced. In the previous publication by Altuna et al, any of those 73 patients underwent Co2TOLMS for early-stage laryngeal cancer included required to be readmitted. 13 Armstrong et al reported an incidence of 0.5% of reintubation after 589 direct laryngoscopies 14 and Whinney et al reported no major complications after 325 rigid endoscopies of the upper aerodigestive tract with less than 1% of readmission rate. 15 Results similar to those reported in this up to date series from our department were 3.8% of the patients needed to be readmitted, and just 1% required to be reintubated.
To prevent high-risk complications, a good clinical and physical examination is essential. Perioperative complications related to Co2TOLMS are extensively described and need to be considered. 16,17 These can be divided into medical or surgical complication. In the first group, we can include the risk of bradycardia or severe respiratory insufficiency. And related to specific surgical complications, the risk of postsurgical bleeding besides the coagulation capacity of the laser and the risk of airway ignition represents the most feared for surgeons, while cervical emphysema due to penetration of the cricothyroid membrane the most significant for patients, followed by tooth damage and mucosal bleeding due to a laceration of the oral cavity mucosa, the lateral pharyngeal wall mucosa, or the lip during suspension laryngoscopy. 16,17
A wordwide need for cost-effectiveness has led many health systems toward inventing new ways and improving techniques and skills in order to achieve better and safer outpatient/day-case health care delivery. Fifteen years ago, our department published an initial experience about the use of CO2TOLMS of the larynx as an outpatients procedure for larynx cancer patients. Due to the previous success, our protocol is still widely used in our department. We need to highlight some limitations in our study that can be the small sample size, the retrospective analysis of our data, the absence of economic analysis, and the lack of control group.
Conclusion
According to our results, CO2TOLMS of the larynx can be safely performed as an outpatient procedure. To establish a proper protocol and to perform a careful preoperative assessment are essential to increase our success rate and to prevent any potential complication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.