
Abstract

Tinnitus is the perception of sound in the absence of an external acoustic stimulus. 1 When there is noise near the ear generated by underlying vascular or other disorders, it is referred to as “objective tinnitus.” Objective tinnitus, especially due to vascular causes, can be diagnosed and treated differently from other types of tinnitus. 2 Therefore, it is important to suspect an objective origin of tinnitus for early detection and appropriate management. A dural arteriovenous fistula (DAVF) is a vascular cause of objective tinnitus. It is an abnormal shunt within the dura, between the arterial and venous system. The location of DAVF and its disruption of the blood flow can produce symptoms such as pulsatile tinnitus, bruit, headaches, visual changes, seizure, cranial nerve palsies, and motor or sensory deficits. We herein report the rare presentation of DAVF supplied by multiple arteries including the right ascending pharyngeal, posterior auricular, and middle meningeal arteries, and both occipital arteries.
A 65-year-old female patient complained of pulsatile tinnitus in the right ear and right-sided retroauricular pain. The symptoms began 2 months prior and were aggravated with head position changes. The patient had no history of head trauma, acoustic trauma, or surgery of the head and neck. Also, she had no other underlying disease. The tinnitus was synchronous with the patient’s heartbeat (“pulsatile”), and occasionally it sounded like something passing by the ear with a stinging sensation. The Tinnitus Handicap Inventory score was 16/100. The patient complained of a lowered quality of life (visual analogue scales [VAS] score 4) and annoyance (VAS score 4) on the tinnitus questionnaire. In the physical examination, there was a humming sound at the right mastoid area with auscultation. Audiologic examinations, including pure tone audiometry, speech audiometry, and tympanometry, were performed and all results were normal. The pain that the patient complained of mainly occurred at the right retroauricular area but it occasionally reached the occipital area. Magnetic resonance imaging (MRI) with angiography (MRA) was performed, and DAVF at the right transverse sinus was found. Four-vessel angiography revealed that the right transverse and sigmoid sinus DAVF was fed by multiple dural branches of the right internal carotid artery, bilateral external carotid artery, and bilateral vertebral artery (Figure 1A and B). Transverse coil embolization of the right transverse and sigmoid venous sinuses and jugular bulb was done (Figure 2A). After embolization, the DAVF flow was remarkably reduced (Figure 2B). Immediately after embolization, tinnitus totally subsided. Although multiple feeding arteries still remained, the embolization was terminated in anticipation of spontaneous regression (Figure 2C). A total of 61 detachable and pushable coils were used for embolization. After embolization, we informed the patient of external manual carotid compression (EMCC) to promote and support spontaneous regression of the lesion. 3 To evaluate the symptoms and complications, regular follow-up was done after embolization. Tinnitus completely disappeared and there was no recurrence until 15 months later. Also, there was no auscultated sound at the mastoid area.
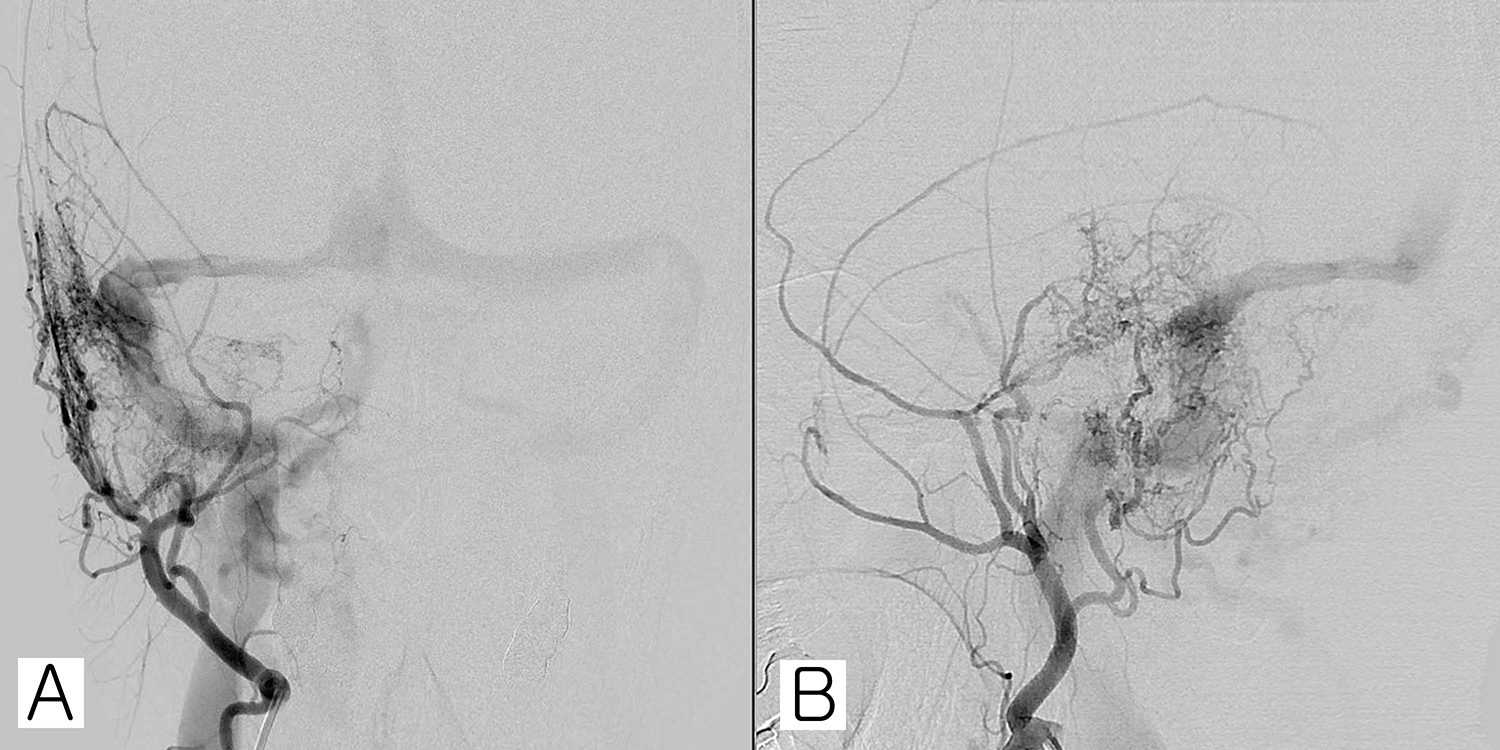
Transfemoral cerebral angiography (TFCA) was performed before embolization. A right transverse and sigmoid sinus dural arteriovenous fistula (DAVF) is found and fed by multiple branches of the bilateral occipital, right ascending pharyngeal, right posterior auricular, right middle meningeal (from bilateral external carotid artery), right lateral tentorial (from right internal carotid artery), and right posterior meningeal arteries (from bilateral vertebral artery). (A) Coronal view. (B) Sagittal view.
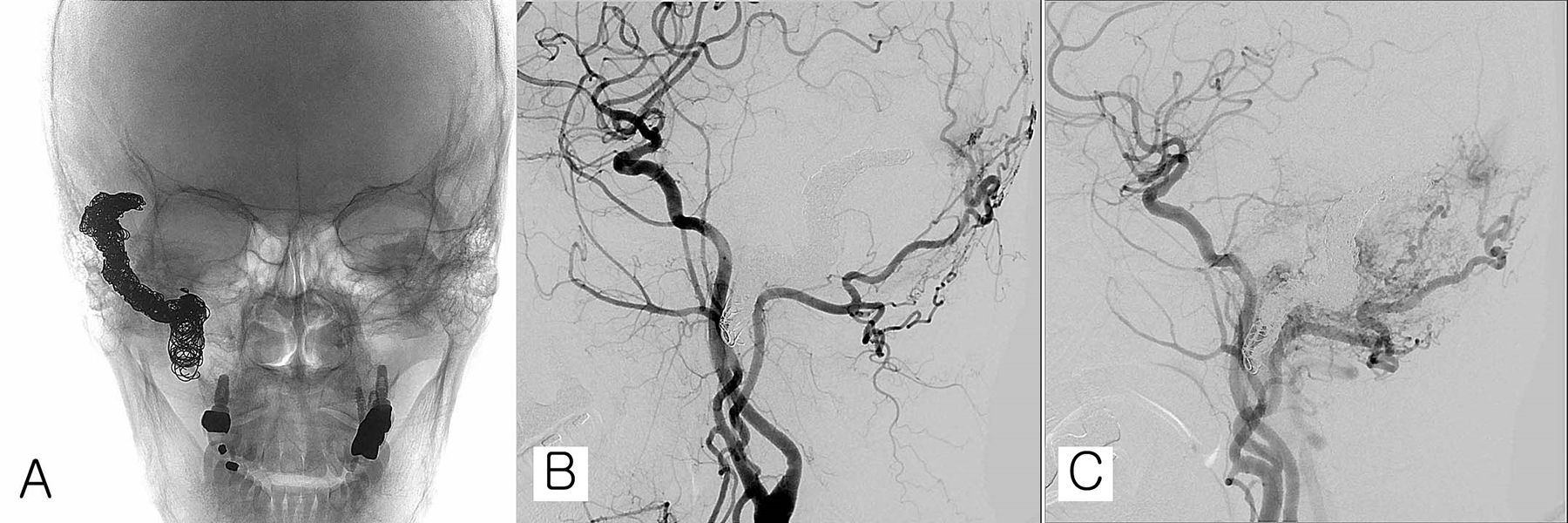
Transfemoral cerebral angiography (TFCA) was performed right after embolization. (A) Coil embolization is performed with 61 detachable and pushable coils. (B) Disappearance of the arteriovenous fistula (AVF) shunt. (C) Residual feeding vessels are identified but expected to disappear spontaneously.
When patients complain of tinnitus, it is important to characterize the tinnitus as objective or subjective. Based on the patient’s description of the tinnitus and physical examinations, including manual compression or rotation of the neck and/or auscultation at the mastoid region or carotid area, additional workup and treatment can be determined. If the sound is synchronous with the heartbeat (“pulsatile tinnitus”) and changes with neck rotation or compression, it is suggestive of a vascular cause. When the cause of tinnitus is suspected to be vascular, noninvasive imaging including computed tomography (CT), CT angiography/venography, MRI or MRA/MR venography is the first choice for diagnosis. And then, digital subtraction angiography is the gold standard to detect and evaluate a suspected DAVF. 4 Dural arteriovenous fistula is a type of vascular malformation that has abnormal communication between the meningeal arteries and dural venous sinuses and/or subarachnoid veins. 4 In symptomatic cases of DAVF, the clinical presentations vary depending on the pattern of venous drainage and location of the fistula. Dural arteriovenous fistula has been managed by conservative therapy, endovascular treatment, surgery, and radiosurgery. The most effective technique is selected depending on the types and clinical presentations of DAVFs. 5 For DAVFs with no improvement after conservative therapy, embolization of the fistula connection and its venous components with an endovascular approach can be the next option of treatment. In addition, EMCC is conducted after embolization to promote and support spontaneous regression of the lesion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by clinical research grant from Pusan National University Hospital in 2020.