
Abstract

A 53-year-old man presented to our otology tertiary referral clinic with left-sided conductive hearing loss after undergoing a left middle fossa craniotomy in another institution. Four months prior, the patient had undergone middle fossa repair of a large dehiscence of the left tegmen tympani and mastoideum by an experienced neurosurgeon. The repair was performed using a free temporalis muscle patch. Immediately after the surgery, the patient reported having ipsilateral hearing loss and was subsequently discharged after recovery without an otoscopic or audiological evaluation. In our center, a noncontrast high-resolution computed tomography scan of the temporal bone was ordered, and the results revealed soft tissue opacification prolapsing through the tegmen defect into the epitympanum in an otherwise aeriated middle ear cleft (Figure 1A). The incus was completely dislocated at the incudomalleolar and incudostapedial joints (Figure 1B and C). The long process of the incus protruded laterally into the external auditory canal (Figure 1D). The otoscopic examination showed a dry central tympanic membrane perforation, with the long incus process protruding laterally into the ear canal (Figure 2). The patient did not suffer from cerebrospinal fluid otorrhea and was neurologically intact, indicating that the tegmen dehiscence had been successfully repaired. His only complaint was the resulting conductive hearing loss. The patient consequently underwent uneventful tympanoplasty surgery with ossicular reconstruction.
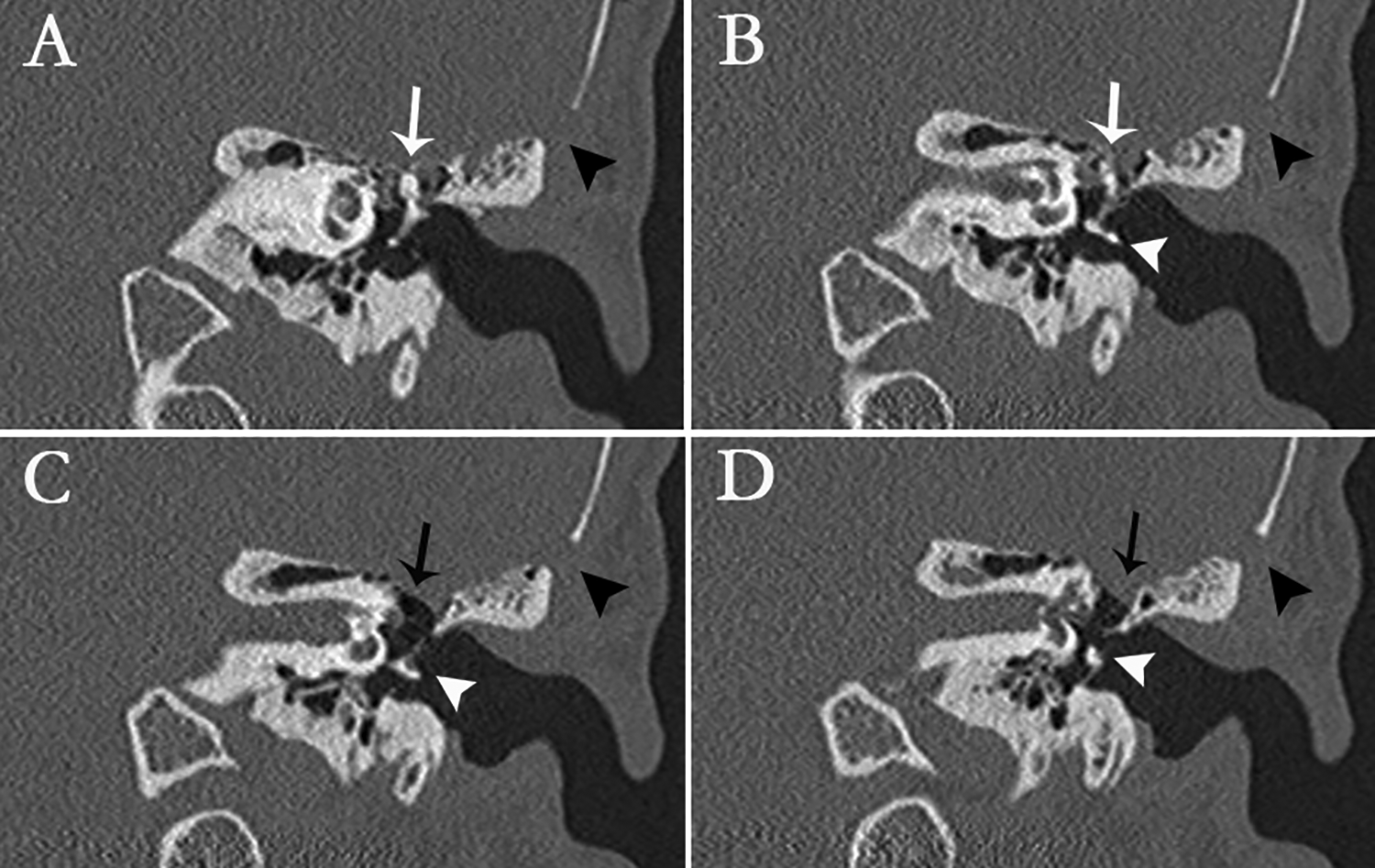
Noncontrast high-resolution computed tomography images of the temporal bone in the coronal plane. The middle cranial fossa craniotomy is visible at the lateral edge of the images (black arrowheads). A and B, The white arrow points to the normally positioned malleus head, which is exposed through the tegmen dehiscence. B, The white arrowhead indicates the dislocated long incus process, which protrudes laterally into the external auditory canal. C and D, The white arrowhead indicates the dislocated body and short process of the incus. The black arrow points to the repair material, shown as soft tissue opacification, protruding inferiorly through the dehiscence into the attic, reaching the level of the lateral semicircular canal.

Otoscopic view of the left tympanic membrane. The malleus appears in the normal anatomical position (black arrowhead). A dry central tympanic membrane perforation can be seen. The long incus process extends laterally through the perforation into the external auditory canal (white arrowhead).
Surgical repair of tegmen dehiscence has been performed using either transmastoid, middle fossa craniotomy or combined approaches.1-4 The middle fossa approach has been deemed particularly suitable for large defects with exposure of the ossicular heads. 2 To our knowledge, this is the first report of traumatic tympanic membrane perforation and incus dislocation into the external auditory canal as a complication of middle fossa repair of tegmen dehiscence. This case highlights the importance of prompt otologic and/or audiologic examination, if patients experience ipsilateral hearing loss postoperatively. Surgeons should be aware of this complication when performing middle fossa repairs of large tegmen defects with exposure of the ossicular heads. Overplugging of the defect should therefore be avoided. A definite diagnosis can be reached using high-resolution temporal bone computed tomography.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.