
Abstract

Introduction
Common midline lesions affecting the pediatric nose include hemangiomas, gliomas, dermoid cysts, and encephaloceles. Radiological assessment is imperative in making the diagnosis.
Patient Presentation
A 1-month-old male presented to the pediatrician anomalies with a soft tissue lesion that completely obstructed the right nasal airway. Physical examination at this stage revealed a firm, noncompressible mass in the posterior nasal space (Figure 1), and computed tomography (CT) scan findings suggested a nasal glial heterotopia (Figure 2). Neurosurgical consultation confirmed that there was no encephalocele.
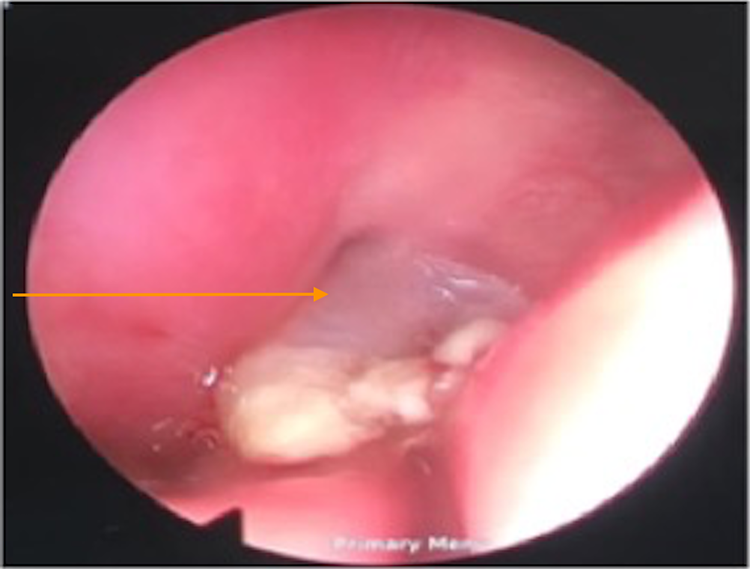
Endoscopic view of nasal mass filling nasopharynx (orange arrow).
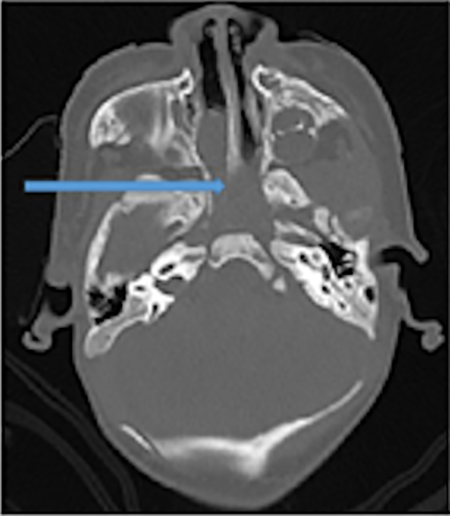
Axial computed tomography (CT) scan showing nasal and nasopharyngeal mass (blue arrow).
The patient underwent endoscopic resection of the nasal tumor. Postoperative the child was monitored in the intensive care unit and then discharged to the paediatric ward.
Histopathology of the mass revealed multiple polypoid fragments, ranging from 18 × 10 × 8 to 7 × 5 × 4 mm. These polypoid fragments were lined by mature stratified squamous epithelium, with underlying nests of heterotopic mature neuroglial tissue present. There was no evidence of a malignant infiltration. Immunostaining confirmed the diagnosis to be glial heterotopia (Figure 3). Postoperative magnetic resonance imaging (MRI) confirmed that indeed the mass was completely removed and there was no communicating encephalocele (Figures 4 and 5).
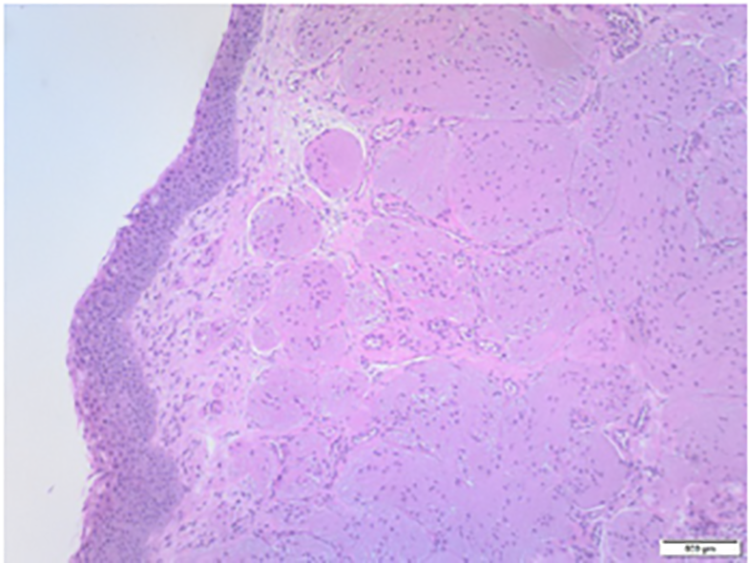
Histology demonstrating nasal glial tissue.
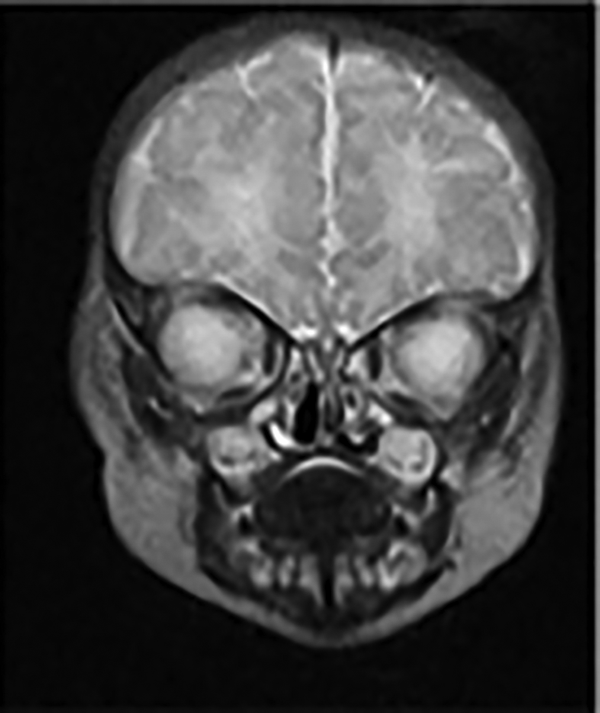
Magnetic resonance imaging (MRI) coronal view postoperative showing intact base of skull.
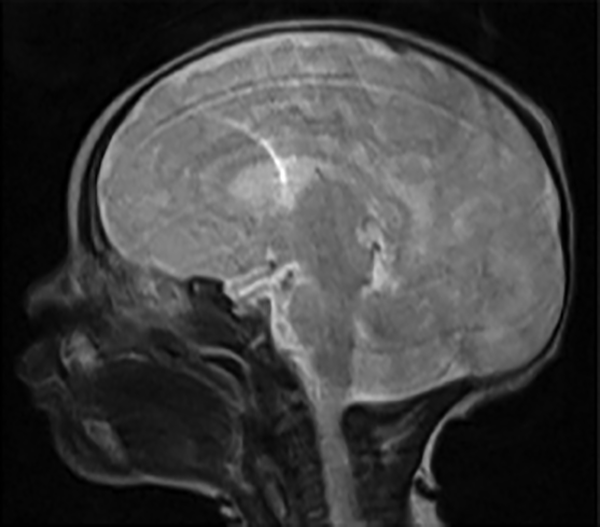
Magnetic resonance imaging (MRI) sagittal view demonstrating no cerebrospinal fluid (CSF) leak or encephalocele.
The recovery period was uncomplicated and the child was discharged. Postoperative visits at 1 and 6 months were satisfactory. The child was breathing well, growing well, and had no residual tissue or recurrence based on flexible nasal endoscopy.
Discussion
Nasal gliomas, encephaloceles, and nasal glial heterotopia predominantly appear in the paediatric population, causing nasal obstruction, difficulty with feeding, and nasal cosmetic deformities. More importantly, these lesions can be a foci of infection. 1
Reid first described the entity of nasal glioma in 1892. Schmidt was the first to present a comprehensive description of this entity and coined the term glioma in 1900. The term implies a true neoplasm and is therefore a misnomer, and because of this some authors have recommended the use of such terms as encephaloma or nasal cerebral heterotopia. 2
These lesions may manifest as: extranasal (60%), intranasal (30%), or combined (10%). 3 Nasal endoscopy is performed to determine the location, origin, and extent of the nasal mass and to assess lack of or presence of pulsation, which is of paramount importance. Needle aspiration or biopsy should be avoided.
The preoperative evaluation must include cross-sectional imaging studies to assess the location, size, and contents of the lesion. The integrity of the anterior skull should be assessed, and herniation of intracranial contents into the nasal region should be documented. Thin-section, high-resolution axial and coronal CT images provide useful information about bony anatomy. 4
In young infants, the anterior skull base is only partially ossified. In this situation, intravenous contrast is used to delineate the cartilaginous skull base. Thin-section, high-resolution multiplanar MRI provides complimentary information to CT regarding the fluid or soft tissue characteristics of the mass. Herniation of meninges alone (meningocele) or brain and meninges (encephalocele) is sometimes apparent. Contrast-enhanced images should be obtained to aid in the differential diagnosis of solid masses.5-7
The proper management of nasal glioma and encephalocele requires a multidisciplinary approach that includes otolaryngology, neurosurgery, and neuroradiology services. Patients should undergo a complete examination to exclude any other congenital abnormalities.8-11
Footnotes
Authors’ Note
All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the University of the Witwatersrand Human Research Ethics Committee. As the patient’s personal details were kept anonymous and no patient images were used, the Helsinki ethical principles were followed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.