
Abstract
Background:
Tympanostomy tube placement is one of the most common surgical procedures performed across the globe. Controversies exist regarding what to do when a tube is considered to be retained in the tympanic membrane for too long.
Materials and Methods:
Review of the PubMed medical literature starting in 1990, focusing on English language studies reporting on the definition, complications, and management of retained tympanostomy tubes.
Results:
The medical literature reporting on outcomes regarding retained tympanostomy tubes is relatively sparse. Most studies recommend prophylactic removal of tubes after a defined period of time, usually around 2 to 3 years after placement. A preferred method of myringoplasty after tympanostomy tube retrieval has not been established, but most studies recommend grafting the perforation at the time of tube removal.
Conclusions:
Although a consensus as to the optimal management of retained tympanostomy tubes is not yet established in the medical literature, a preponderance of studies recommend prophylactic removal at defined period of time (>2-3 years) before the onset of complications such as otorrhea and granulation tissue formation. Due to a lack of best evidence, the surgeon’s preference remains the guiding principle as to the best technique for myringoplasty at the time of removal.
Introduction
In the United States, the use of tympanostomy tubes for the management of otitis media remains one of the most common surgeries in the pediatric community. Reasons for the use of tubes depend on varied factors, but most commonly include persistent middle ear fluid with associated risk factors, recurrent acute otitis media, or complicated otitis media. 1 It is common for most tympanostomy tube types to spontaneously extrude after 6 to 18 months with complete healing of the tympanic membrane (TM). 2 However, if the tube has not fallen out after a certain amount of time (usually 2 years), it is considered “retained” and one must consider whether the patient should have these removed. Although studies are lacking on the subject, conventional and empirical evidence would suggest that the process of TM epithelial migration and re-epithelialization is indeed what leads to tympanostomy tube extrusion. Concerns regarding complications of retained tympanostomy tubes have been brought to light and include persistent TM perforation, persistent otorrhea, formation of granulation tissue, or growth of cholesteatomas. 3 Controversies exist as to the expected outcomes from retained tube removal when the patient is asymptomatic, rather than removal due to complications. 2,4,5 This review will summarize and synthesize the literature on the topic of retained tympanostomy tubes in the pediatric population as well as offer suggestions based on findings in the literature in conjunction with the senior author’s experience as a pediatric otolaryngologist at an academic children’s hospital. Table 1 provides a brief synopsis of all studies identified and reviewed herein.
A Synopsis of Studies Included in This Paper Showing the Findings Related to Retained Tubes and the Removal of Retained Tubes as Well as Different Mechanisms of Tympanic Membrane (TM) Repair.
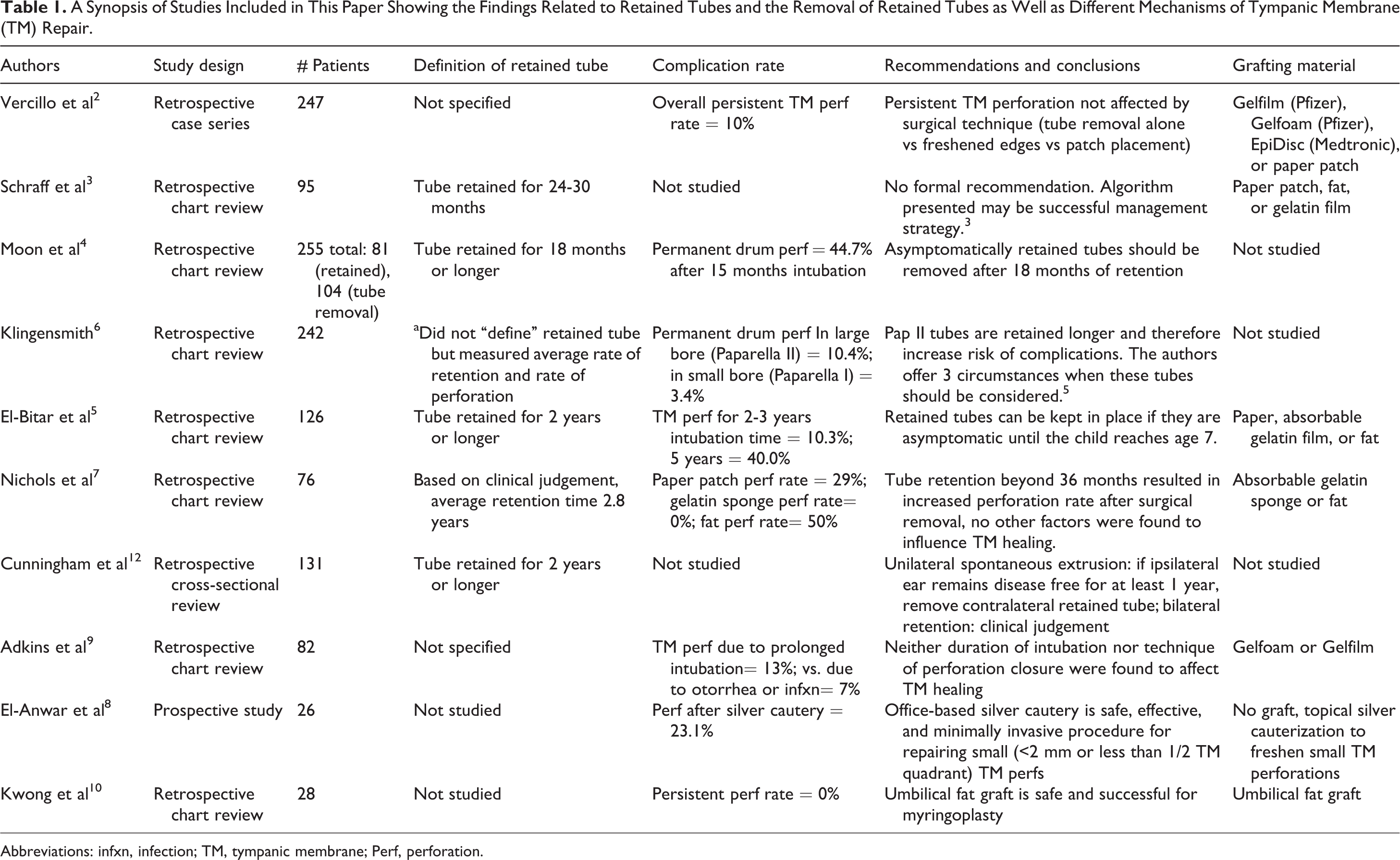
Abbreviations: infxn, infection; TM, tympanic membrane; Perf, perforation.
Methods
A review of medical literature beginning in the year 1990 was conducted via PubMed. Search terms included or were related to “retained tympanostomy tubes,” “tympanostomy tube complications,” and “tympanic membrane repair after tympanostomy tube removal.” Additional publications were found via the references of reviewed literature. The search was focused on the pediatric population; however, no specific search terms were used to specify this, as the majority of retained tympanostomy tube literature pertains to this population. However, the literature focusing on only adult patients was excluded. In addition, the senior author offered personal expertise in terms of management strategies, as there are no specific guidelines on the management of children with retained tympanostomy tubes.
Results/Discussion
Retained Tympanostomy Tubes, What
Although various definitions are referenced in the literature, a tympanostomy tube that does not spontaneously extrude after approximately 2 years can be considered retained. It should be noted that this review focuses on retained tympanostomy tubes in the pediatric population and adult management can vary. Given long-term Eustachian dysfunction as an etiologic factor for the need of tympanostomy tubes in adults, a persistent small perforation may not be repaired. Moreover, adults receiving tympanostomy tubes will often have tympanostomy tubes placed which are meant to last longer than 2 to 3 years, such as T-tubes.
Retained Tympanostomy Tubes, When and Who to Treat
Understanding the effectiveness related to the length of time that tubes remain in the TM, as well as the drawbacks associated, is vital to promoting healthy middle ear function in children. Studies have stated that removing tympanostomy tubes too early can lead to a resurgence of otitis media with effusion, but on the other hand, leaving the tubes in longer than necessary can lead to tube site infection, permanent TM perforation, and cholesteatoma formation. 4,6 Certain factors, such as the age of the patient and length of tube intubation, have been proven to affect the success of a tympanostomy tube in terms of its effectiveness in decreasing the rate of middle ear effusion or need for subsequent tubes in the future. In a study by Schraff et al, TM perforations following tympanostomy tube removal at several intervals were reviewed. They found that 73% of TM perforations were caused by a retained tube left in the ear for 2 years or longer. 3 Moon et al found that the rate of permanent TM perforation, granulation tissue, or discharge near the tympanostomy tubes significantly increased after 15 months from insertion. 4 This same study also found that the rate of recurrence of otitis media with effusion, and the need to reinsert tubes, increased if the tubes were removed before 12 months of intubation, 4 leading this team to conclude that tubes should be removed if they have not spontaneously extruded by 18 months post-intubation. 4 El-Bitar et al conducted a retrospective study of 126 children with tubes that were retained for 2 years or longer and found an increase in complication rates of granulation tissue formation, otorrhea, and permanent TM perforation as the time of retention increased. Additionally, this study found that children older than 7 years have a higher incidence of complications than their younger counterparts; however, the increase in time of retention remains significant in predicting complications throughout all age groups. 5 Nichols et al conducted a retrospective chart review of 76 patients under the age of 12 and found that the rate of TM perforation was higher in children with tubes that had been retained for greater than 3 years. 7 Although no guidelines exist regarding the management of retained tympanostomy tubes past 2 years in children, it is the opinion of the senior author that as long as there is no associated secondary inflammatory reaction such as granulation tissue or recurrent otorrhea not responding to ototopicals, the patient can be safely followed every 6 to 8 months to allow for spontaneous extrusion of the tube. The risk of a second anesthesia required to remove the tube must be balanced with the risk of allowing the tube to remain in the TM over the long run.
Retained Tympanostomy Tubes, How to Treat
There are a variety of techniques for tympanostomy tube removal and subsequent closure of the TM, including freshening of the TM perforation edges, patch myringoplasty, the combination of the 2, or only removing the tube without further intervention. Freshening involves stripping of the TM perforation edges in order to promote granulation tissue and new tissue formation at the perforation site. 8 Myringoplasty involves the closure of the TM with a patch of varying materials including fascia, fat, gelfoam, gelfilm, and engineered biomaterials.
Vercillo et al found no difference in TM healing among different techniques with a total perforation rate of 10%. 2 However, this study notes that variables other than technique such as older age, longer-acting T-tubes, and trisomy 21 were found to negatively impact TM closure. Similarly, Adkins et al found no difference in TM closure among techniques with an overall perforation rate of 13%; however, in this study, the age of the patient was not found to have an effect on TM closure. 9 Despite multiple studies reporting no significant differences amongst types of TM repair, certain novel substances have been proposed to help increase the overall success rate of these procedures including umbilical fat, silk fibroin scaffold, and other biomaterials. 10,11 Ultimately, the decision of TM repair method is surgeon- and patient-dependent. Variables that a surgeon may take into account include size of the perforation, location of the perforation, and personal experience with different approaches or graft types. No guidelines exist in this regard.
Retained Tympanostomy Tubes, Why to Treat
Tympanostomy tube removal may be performed for many reasons; however, the literature supports that the most common indication is due to retained tubes as defined above. The removal of retained tympanostomy tubes is considered due to the risk of developing complications, some of which require surgical repair and can impair hearing. There are no specific guidelines on removal of retained tubes. However, previous literature supports that higher complication rates are observed in children with tubes that are retained for greater periods of time among all pediatric age groups. 5,12 There are 2 groups of patients in which the otolaryngologist must consider the removal of a retained tympanostomy tube—those who are asymptomatic and those who are experiencing a complication from their tube such as otorrhea, infection, or granulation tissue that is not responsive to medication. The debate is more profound in asymptomatic patients—why place a patient under anesthesia with operative risk when there are currently no adverse symptoms?
Persistent TM perforation is one of the most feared and common complications related to tympanostomy tubes, especially in those that have failed to extrude. However, this is controversial, as some studies suggest that retained tubes may not pose greater risk in TM perforation than any other indication for removal. In a retrospective case series of 247 pediatric patients undergoing tube removal, no difference in perforation rate was found among indications for tube removal including retained tube, otorrhea, or both. 2 However, other studies show that the longer the tubes are retained, the more likely one is to develop complications including TM perforation. 4,5 Therefore, even if a patient has not experienced complications from their tympanostomy tubes, it still may be wise to remove the tubes to prevent the development of complications.
Complications such as permanent TM perforation require an additional operation to close the defect and can impair the patient’s hearing. However, permanent TM perforation is also a potential complication of tympanostomy tube removal, so the likelihood of this must be weighed against the likelihood and severity of possible complications. To this point, Adkins et al found that rates of permanent TM perforation did not differ between duration of intubation. 9 As such, there is not a consensus in the literature as to the timing for removal of retained tympanostomy tubes in asymptomatic patients. There are currently no studies in the literature examining the difference in TM perforation rate between tubes that spontaneously extrude versus manually removed tubes.
Tube extrusion into the middle ear is another feared complication of tympanostomy tubes and another reason why asymptomatic tubes should be removed. However, in the case of middle ear extrusion of the tympanostomy tube, the consensus seems to be prompt removal of the displaced tube. Cunningham et al described the displacement of tympanostomy tubes into the middle ear in 6 of 131 ears with retained tubes and, in agreement with other literature, recommend the prompt removal of medialized tubes. 12 Mukerji highlights a case of middle ear tube extrusion and similarly concludes that tubes that have made their way into the middle ear should be removed and treated as a foreign body, even if the child is asymptomatic. 13
Conclusion
Although a consensus as to the optimal management of retained tympanostomy tubes is not yet established in the medical literature, a preponderance of studies recommend prophylactic removal at a defined period of time (>2-3 years) before the onset of complications such as otorrhea and granulation tissue formation. Due to a lack best evidence, surgeon’s preference remains the guiding principle as to best techniques for myringoplasty at the time of removal.
Footnotes
Authors’ Note
The corresponding author had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.