
Abstract

Case
A 78-year-old female presented with a nasopharyngeal branchial cyst incidentally discovered on magnetic resonance imaging (MRI) for evaluation of right-sided headaches. A careful history revealed complaints of occasional right-sided aural fullness. T2-weighted MRI revealed a 2 × 1 × 1 cm hyperintense mass extending along the Eustachian tube and abutting the parapharyngeal internal carotid artery (Figure 1). Nasopharyngoscopy revealed a pulsatile right-sided nasopharyngeal mass effacing the fossa of Rosenmuller with mass effect on the Eustachian tube orifice. She underwent an endoscopic-assisted biopsy with marsupialization of the nasopharyngeal cyst using a 4-mm PROPEL mini mometasone-eluting sinus stent (Intersect ENT Inc).
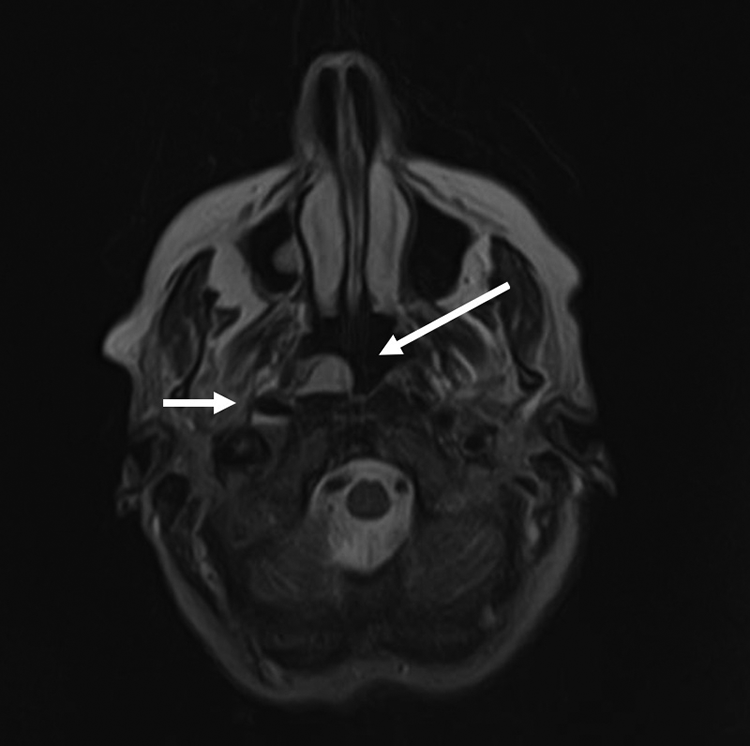
On T2-weighted postcontrast MRI, a 2 × 1 × 1 cm hyperintense mass extending into the parapharyngeal space but not invading the prevertebral fascia was identified (long white arrow). The parapharyngeal internal carotid artery (short white arrow) is abutting the cyst. MRI indicates magnetic resonance imaging.
A small posterior septectomy was performed to achieve enough room for a 2-surgeon, bimanual approach. The posterior septum mucosa was incised with an extended needle-tip Bovie. The mucosa was elevated and removed with through-cutting forceps. The posterior vomer was removed with back-biting forceps while hemostasis was achieved with suction cautery.
The cyst wall was identified and examined for any masses or abnormalities via blunt dissection. Given the proximity to the carotid artery and the benign nature of the cyst, marsupialization was performed. The medial aspect of the cyst wall was incised with cautery revealing thick mucoid contents. An elliptical section of the medial wall was removed using 2 incisions. The first was made along the posterior pharyngeal wall into the retropharyngeal fascia. A second lateral incision was made just posterior to the salpingopharyngeal fold (Figure 2). The cyst wall was sent to pathology. A 4-mm Propel mini sinus implant (Intersent ENT Inc) was placed within the cyst cavity and positioned to maintain patency using the angle Blakesley forceps to promote epithelization and permanent marsupialization.
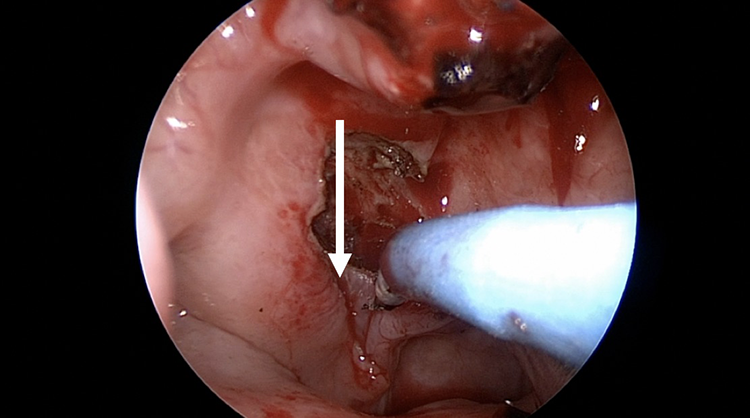
The cyst wall is removed laterally along the salpingopharyngeal fold (white arrow) with a needle-tip Bovie.
The patient was discharged on the day of surgery without complications. She was advised to use Afrin nasal spray for 3 days following surgery and start nasal saline irrigations beginning 1 week after surgery. She had mild aural fullness and expected postoperative minor epistaxis in the first few days. On nasal endoscopy at 1 week, the stent was visualized in place within the marsupialized fossa of Rosenmuller. At 1-month follow-up, the stent had dissolved and the marsupialized cyst was patent (Figure 3).
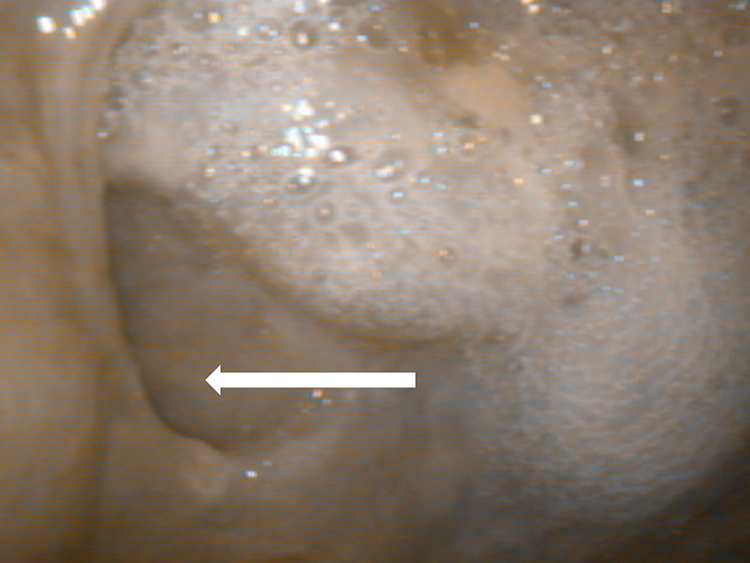
Nasal endoscopy shows the nasopharyngeal cyst cavity (white arrow) remained marsupialized and the stent is dissolved.
Discussion
Lateral nasopharyngeal cysts are rare and are of branchial cleft origin. 1 The treatment is surgery. Regardless of how nasopharyngeal cysts are treated, the common goal for all techniques is to reduce mass effect symptoms, rule out malignancy, and minimize cyst recurrence and bleeding. Techniques to treat nasopharyngeal cysts include aspiration, excision, or marsupialization. Several series have reported successes at minimally invasive endoscopic/robotic approaches.1-4
Advantages to endoscopic cyst marsupialization include decreased risk of injury to the internal carotid artery and lowered risk of cyst recurrence compared to aspiration. Transnasal endoscopic marsupialization of a nasopharyngeal cyst has been previously described using an endoscopic-guided diode laser for marsupialization and reported no cyst recurrence 6 months postoperatively. 2 Transnasal marsupialization has been reported with benefits including improved cosmetic appearance, fewer wound-related complications, and pain compared to transoral transpalatal approaches.1-3
In conclusion, transnasal endoscopic marsupialization of nasopharyngeal cysts is feasible and provides excellent cosmetic and functional results. A 2-handed surgical technique allows for precise excision of the lining, preservation of the Eustachian tube function, and avoidance of the internal carotid injury at the lateral aspect of the cyst. We also describe the novel use of a steroid-eluting mini stent to maintain patency of the marsupialized cyst postoperatively. These stents are absorbable, do not require removal, and provide the patient with little need of postoperative care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.