
Abstract

The cochlear aperture (CA), also known as modiolar base, is the bony opening at the base of the modiolus that transmits blood vessels and nerve fibers from the spiral ganglion to the cochlear nerve. The short canal through which the cochlear nerve passes from the fundus of the internal auditory canal (IAC) into this aperture is referred to as the bony cochlear nerve canal (BCNC). Cochlear aperture, modiolar base, and BCNC are often used interchangeably in the literature.
Through small reports and series, enlarged cochlear aperture (ECA) has now been associated with a greater risk for hearing loss and surgical complications. To date, cases of ECA have been described in patients with X-linked deafness 1 or in association with other radiographic malformations such as incomplete partition-II, bony dehiscence, or enlarged IAC. 2 We report a unique case in which a child with negative genetic testing and radiographically normal ears underwent sequential cochlear implantation (CI) for congenital deafness. During both procedures, cerebrospinal fluid (CSF) gushers were encountered. On review of imaging, bilateral ECAs were identified. The goals of this report are to emphasize ECA as a risk factor for intraoperative CSF gusher and underscore the importance of identifying ECA even in radiographically normal ears.
A 13-month-old boy with hypothalamic hamartoma and sickle cell anemia had been followed for congenital hearing loss at a tertiary care referral center. He had failed newborn hearing screening, and subsequent testing was indicative of a severe-to-profound bilateral sensorineural hearing loss. A complete genetic workup and family history was unremarkable. Preoperative high-resolution computed tomography scans of the temporal bones were read as normal on outside studies (Figure 1).
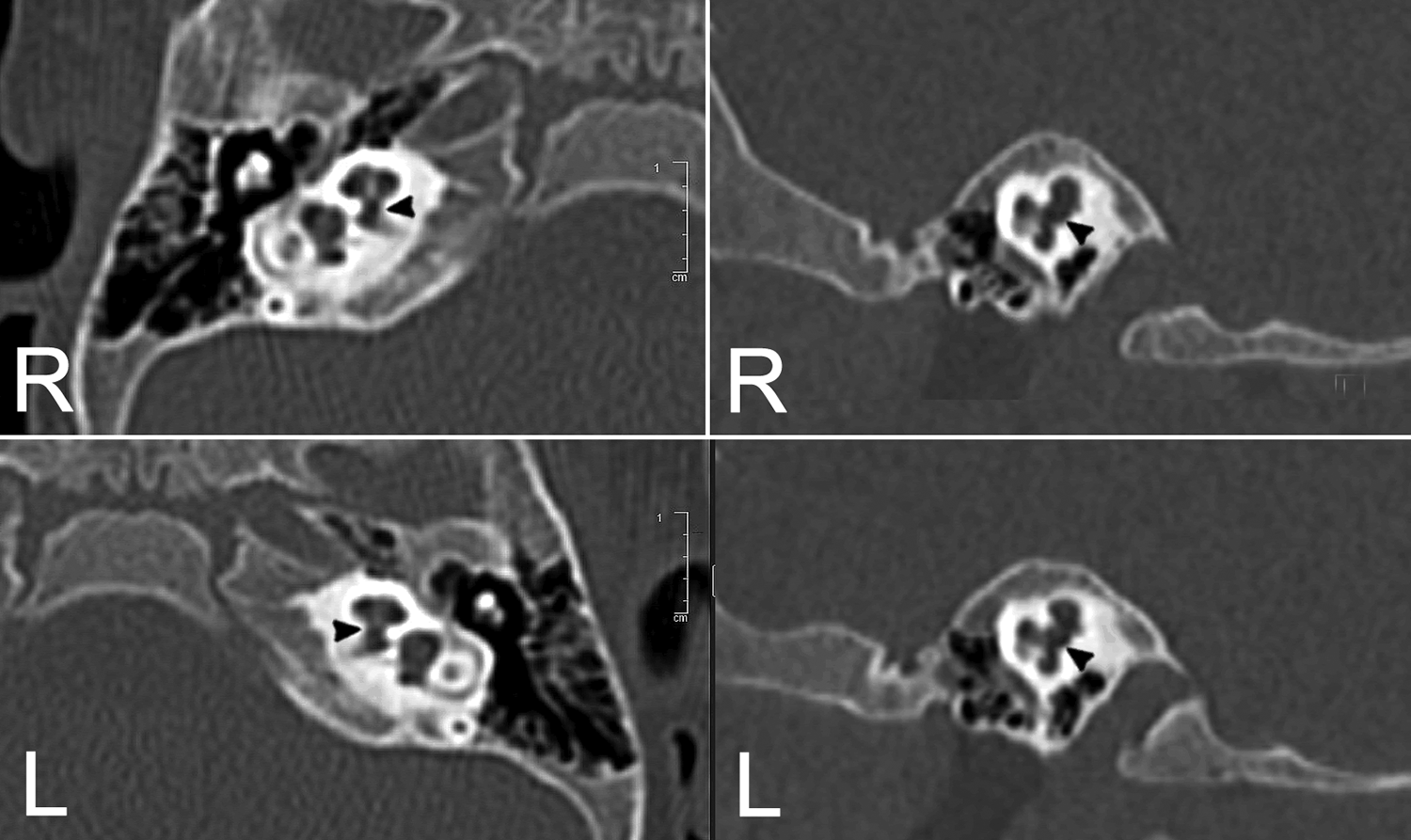
Temporal Bone Imaging. Axial (left) and sagittal (right) noncontrast temporal bone scans. Bilateral enlarged cochlear apertures (black arrowheads) are seen entering the cochlea. The right cochlear aperture measured 2.3 mm and the left cochlear aperture measured 2.4 mm.
His right ear was implanted first with a Cochlear Nucleus CI 522 (Cochlear Ltd). Upon performing the cochleostomy, a CSF gusher was encountered. Temporalis muscle, fascia, and Surgicel (Ethicon) were used to pack the cochleostomy around the electrode. Tisseal (Baxter Inc) was used in the facial recess. Postoperative course was uneventful with no meningitis or persistent CSF leak. A lumbar drain was not required. After encountering the CSF gusher, a rereview of the imaging was performed, and a finding of ECA was identified. Fourteen months later, the patient underwent a left CI with an identical implant. A high-flow CSF gusher was once again encountered following the creation of the cochleostomy and was repaired identically (Figure 2). Postoperative course was again uncomplicated. In his most recent follow-up, the patient has demonstrated excellent benefit from his cochlear implants with expected gains in speech-language development.
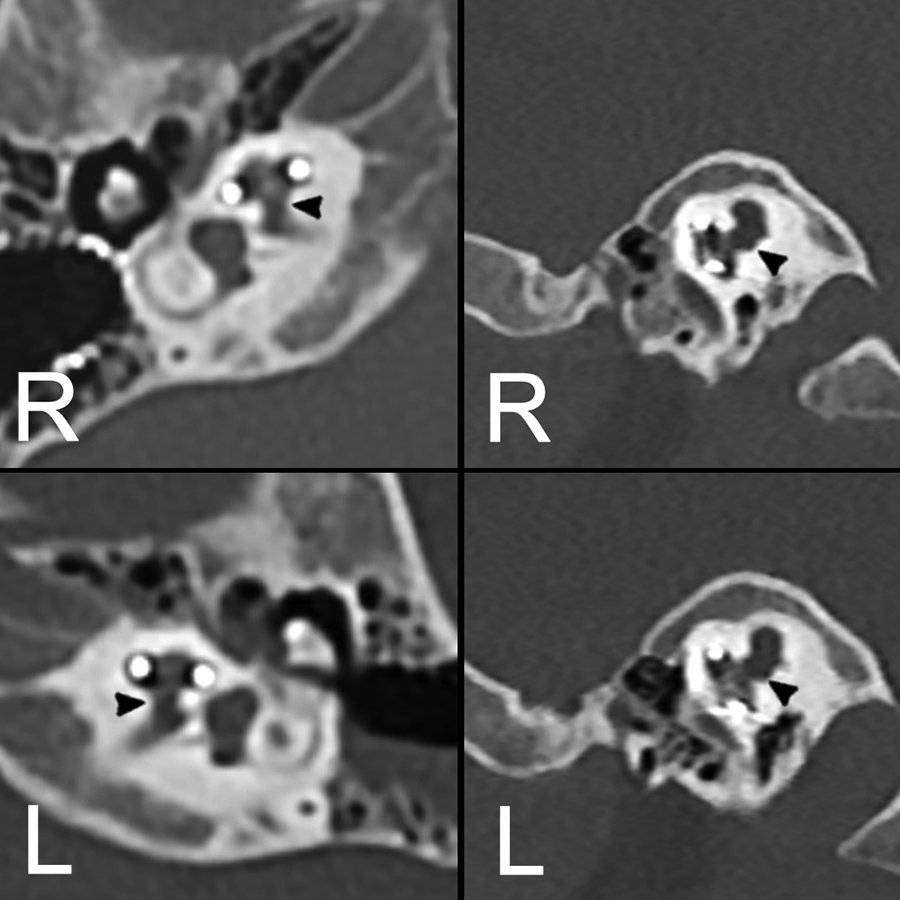
Postoperative Imaging. Axial (left) and sagittal (right) noncontrast temporal bone scans after sequential cochlear implantation. Cochlear implant electrode arrays are seen in proper position.
Cerebrospinal fluid leaks occur in approximately 1% of pediatric cochlear implant surgeries. In our patient, both CSF gushers required over 30 minutes to control and increased operative time by over 50%. Fortunately, there were no postoperative sequelae. Our patient had normal IAC diameters and was without other inner ear malformations. In this case, the probability of bilateral spontaneous CSF gushers with no other risk factor would have been exceedingly low.
Although size criteria for ECA are not well defined, both CAs in our patients were considered enlarged. In his original paper from 1999, Fatterpekar et al studied the temporal bone scans of 50 normal hearing individuals and found the average CA diameter to be 2.13 mm. 3 Recent data are consistent with these findings. In one of the largest imaging series of 100 healthy controls, the average CA was found to be 1.91 mm. 4 In our patient, the right CA measured 2.3 mm and left measured 2.4 mm. Wider communication from an enlarged aperture generates larger gradients in hydrostatic pressure between the subarachnoid space and cochlear modiolus, which may lead to CSF gushers.
Although we report an uncommon surgical complication associated with an even rarer anatomic abnormality, its identification has prognostic significance and critical implications in preoperative counseling. Temporal bone imaging has an important role in identifying inner ear abnormalities, and systematic review thereof is critical.
Footnotes
Authors’ Note
This work was presented at the Triological Society Virtual Poster Session of the Combined Otolaryngology Spring Meetings, May 15 to June 14, 2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.