
Abstract
Otophyma is a rare condition that can result in conductive hearing loss. Current otophyma literature does not examine validated treatment outcomes for patients. Utilizing a medical and surgical approach to maintain a patent canal can lead to significant objective improvements. The aim of this case series is to describe a combined successful approach in 3 cases from an academic, multidisciplinary center. The main outcomes analyzed were pre and post air-bone gap audiogram analysis and disimpaction frequency. The results showed that post-management, patient 1 had substantial improvement in hearing, recovering 49 dB in his right ear and 25 dB in his left ear, demonstrating near complete air-bone gap closure. Patient 2 showed a similar dermatologic and functional improvement, although objective audiometric assessment related to otophyma could not be performed due to coexisting chronic otitis media and cholesteatoma. Patient 3, in the 12 months prior to comanagement, had 8 bilateral disimpactions, and following comanagement had 2 disimpactions in 23 months. All 3 patients were pleased with the resultant functional and physical appearance following comanagement. By presenting this approach and objective measures of treatment, we hope to improve future clinical decision-making in a rare condition.
Introduction
Otophyma is a poorly referenced condition, associated with other phymatous changes of rosacea (see Table 1 for literature review). We present 3 otophyma cases with associated hearing abnormalities, rosacea, and rhinophyma, to describe a combined surgical and medical management approach.
Review of Current Literature Regarding Otophyma.a
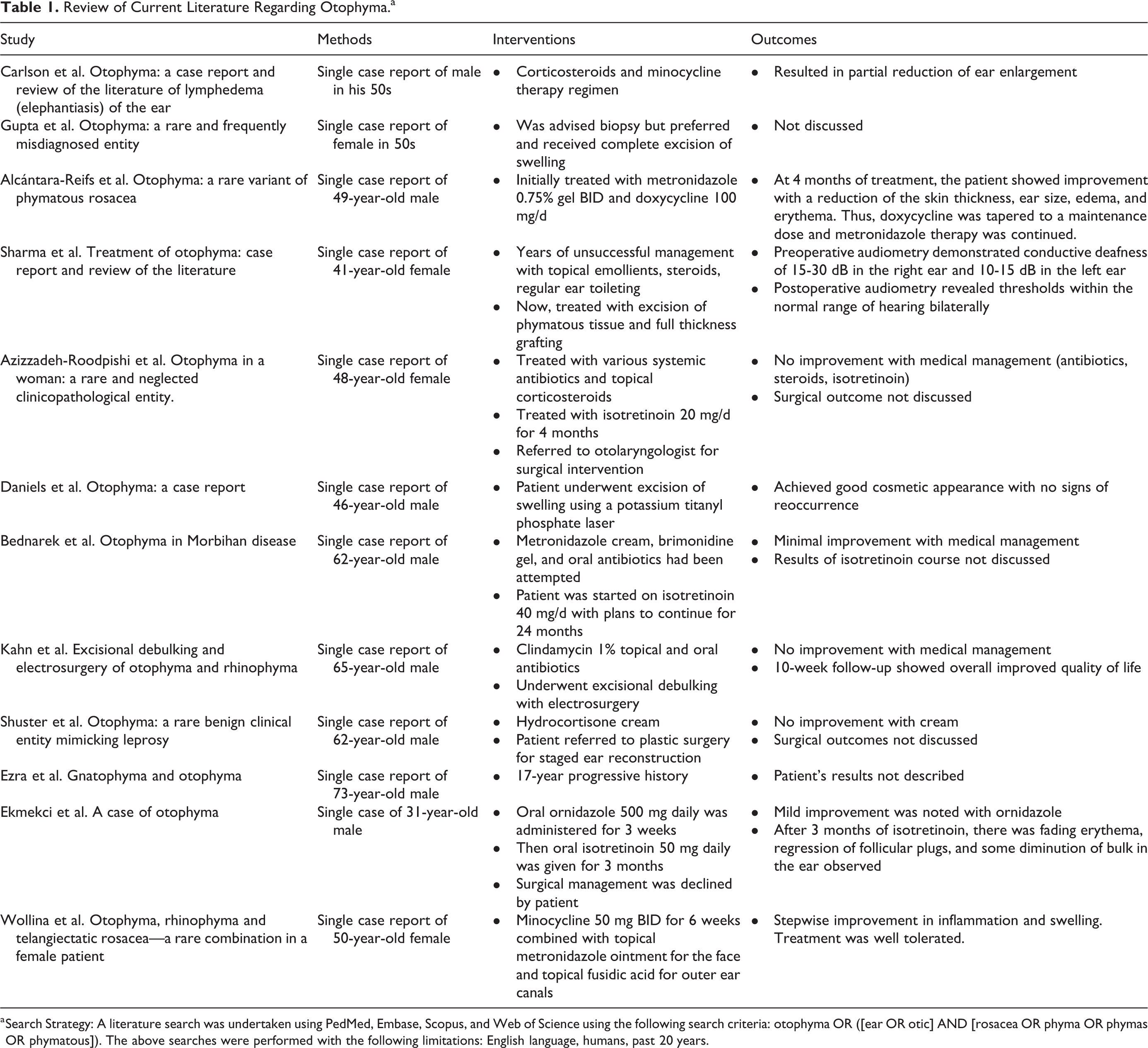
a Search Strategy: A literature search was undertaken using PedMed, Embase, Scopus, and Web of Science using the following search criteria: otophyma OR ([ear OR otic] AND [rosacea OR phyma OR phymas OR phymatous]). The above searches were performed with the following limitations: English language, humans, past 20 years.
Case Reports
A male in his 40s presented to dermatology with a 20+ year history of bilateral ear phymatous changes complicated by progressive hearing loss (Figure 1). After multiple biopsies and diagnoses, the patient underwent bilateral canaloplasty and meatoplasty leading to significant improvement and was started on isotretinoin for long-term management (see Table 2).
Presenting 3 Case Reports Examining Outcomes of Comanagement.
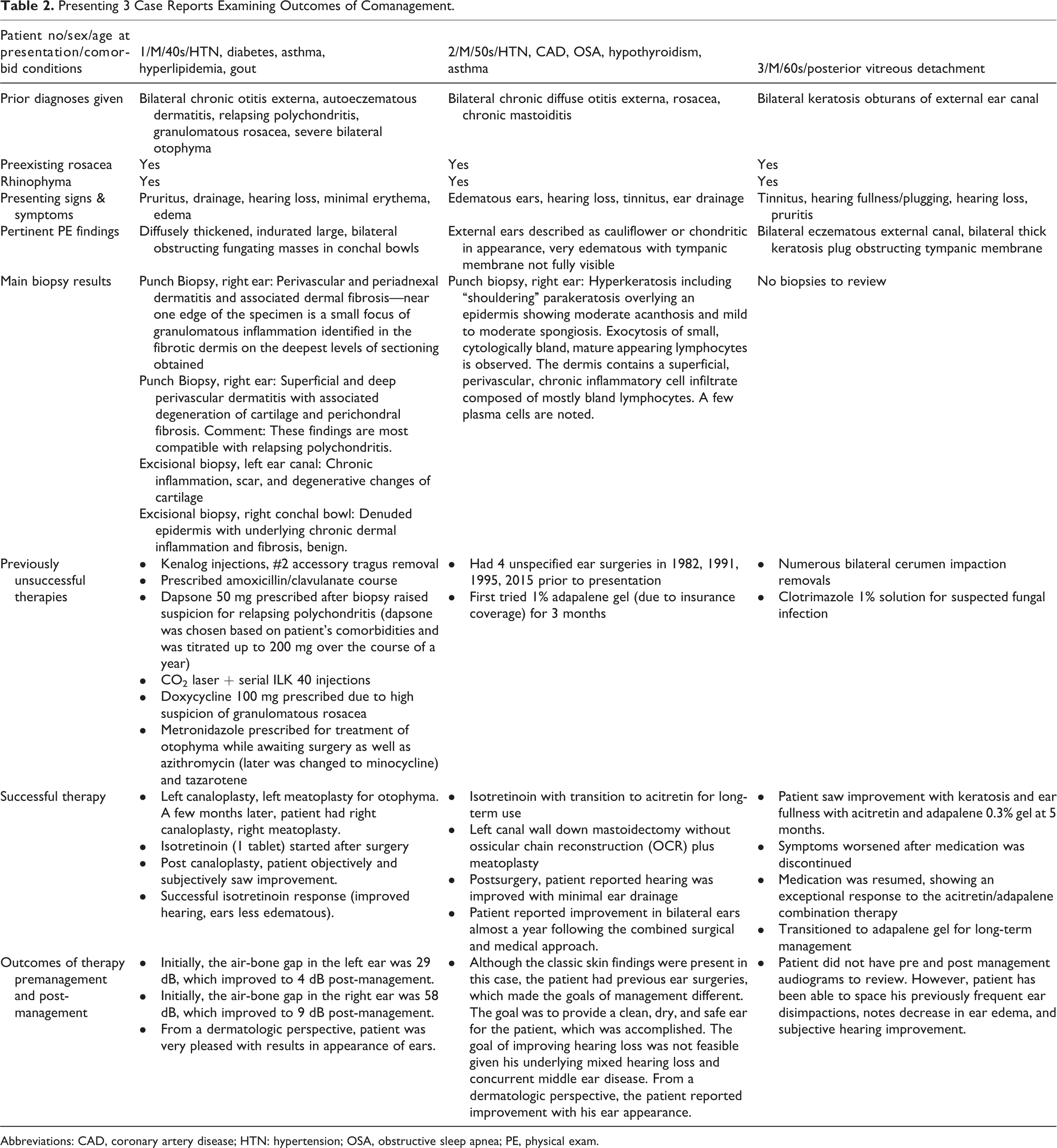
Abbreviations: CAD, coronary artery disease; HTN: hypertension; OSA, obstructive sleep apnea; PE, physical exam.

Left: preoperative photo, post lidocaine injection of patient one’s left ear. Right: postoperative follow-up photo of patient one’s left ear.
A male in his 50s presented to otolaryngology with bilateral hearing loss. He was referred to dermatology for isotretinoin, which reduced his ear edema, after which he underwent left mastoidectomy for associated chronic otitis media and cholesteatoma. Due to concerns with recurrence, he was transitioned to acitretin for long-term management.
A male in his 60s presented to otolaryngology with bilateral enlarged auricles and canal stenosis, which required monthly cerumen disimpactions. After 6 months of acitretin and adapalene 0.3% gel therapy, he noted subjective hearing improvement, fewer disimpactions, and was transitioned to adapalene gel for long-term management.
Discussion
Otophyma describes unilateral or bilateral ear enlargement characterized by fibrosis, sebaceous hyperplasia, and edema. 1 These phymatous changes occur in the outer third of the external auditory canal (EAC) where the sebaceous glands reside. While otophyma is poorly cited, there are several cases of bilateral ear enlargement with biopsies supporting the diagnosis of otophyma. 1 -12 These patients were treated with a variety of medical therapies including metronidazole, doxycycline, dapsone, and prednisone without objective verification of improvement. Most literature emphasizes including otophyma in the differential for ear enlargement. The differential is broad encompassing other edematous conditions including relapsing polychondritis, chronic dermatitis, and chronic otitis externa. 12 Consequently, many patients go through an extensive workup receiving antibiotic and steroid treatments before the final otophyma diagnosis is made. In most case reports, medical management fails, resulting in debulking surgery (excisions, laser techniques, skin grafting) with mixed outcomes. 10
Unlike rhinophyma, conductive hearing loss from accumulation of desquamated debris or soft tissue stenosis of the EAC is a potential sequelae of otophyma. Pre and post-management audiograms can be used to measure outcomes and highlight the importance of comanagement between a dermatologist and an otolaryngologist. Specifically, examining the change in the air-bone gap as well as disimpaction frequencies can provide an objective verification of improvement in combination with the dermatologic and subjective improvements.
The comanagement approach relies upon canaloplasty to promote a self-cleaning ear followed by retinoid therapy, which acts 2-fold: to diminish the size and activity of sebaceous glands and to downregulate the inflammatory response by interfering with leukocyte chemotaxis. 1,13 After this combined approach, our first patient had near complete closure of the air-bone gap bilaterally, signifying a substantial recovery of conductive hearing loss, improving by 49 dB in his right ear and 25 dB in his left ear. In contrast, the second patient had underlying middle ear disease with mixed hearing loss, distinct from his otophyma presentation. This complicated his posttreatment audiogram interpretation. Nonetheless, this case had a successful outcome indicated by a dry and patent ear canal and the patient’s ability to wear hearing aids without further inflammation or infection. The third patient did not have pre and post-management audiograms to compare; however, given the extensive frequency and large amount of debris removed during his disimpactions, it can be presumed he had some degree of conductive hearing loss. The patient did however have a marked improvement in his disimpaction frequencies. In the 12 months prior to comanagement, the patient had 8 bilateral disimpactions. In the 23 months post-management, he has required only 2 disimpactions and reports hearing improvement. All 3 patients were pleased with the resultant functional and physical appearance following this comanagement approach.
Footnotes
Author’ Note
The data that support the findings of this study are available from the corresponding author, MMP, upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.