
Abstract

A 28-year-old woman visited our department due to a 1-month history of severe otalgia of the left ear. She complained of developing taste loss in her left tongue 2 weeks later. Upon a physical examination, a hyperdense and cerumen-like material was discovered plugged in her left external auditory canal (EAC; Figure 1A). High-resolution computed tomography of the temporal bone indicated a nodule-like lesion in the left EAC, abutting the left tympanic membrane (Figure 2). The lesion was removed completely through endoscopy under general anesthesia, and the operative findings revealed a widened EAC with expansion to the hypotympanum (Figure 1B). The pathology was compatible with keratosis obturans (KO). After 3 weeks postoperatively, the wound healed spontaneously with exposure of the chorda tympanic nerve (Figure 1C). Despite no recurrence, the patient had persistent taste loss after 3-month follow-up.
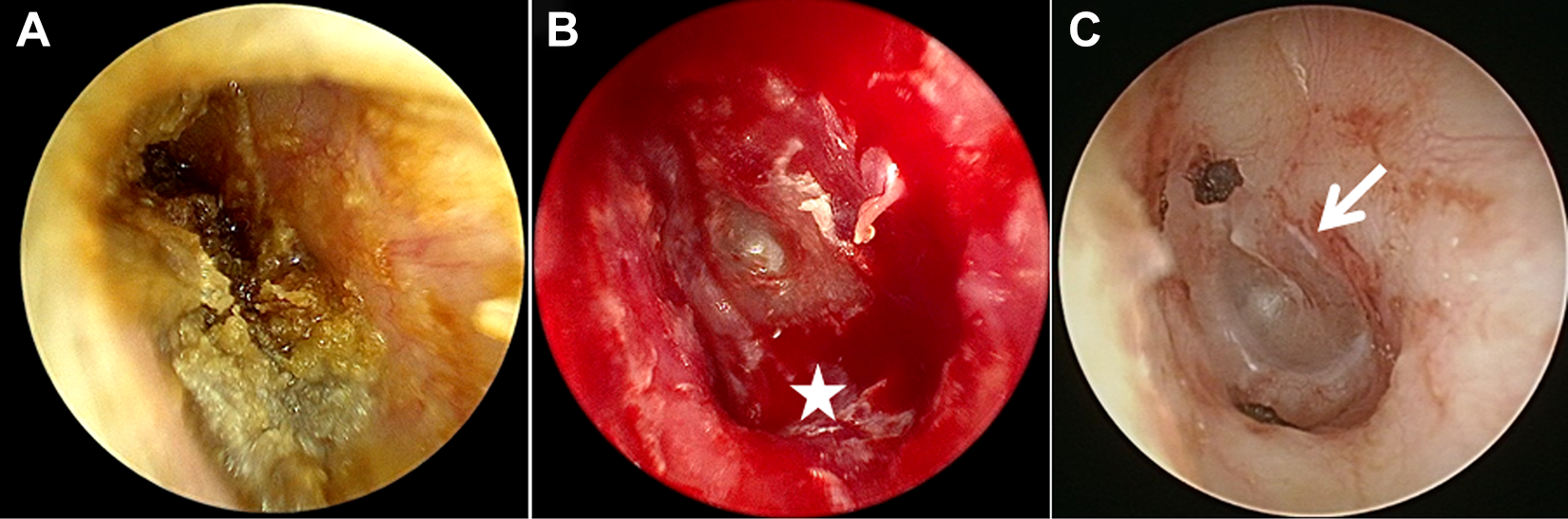
A, Otoscope showing hyperdense and cerumen-like materials plugged in the left EAC. B, After removing the lesion, the otoscope showed a widened canal with expansion to the hypotympanum (star) without eardrum involvement. C, At 3-month follow-up, the skin healed with a widening canal in the deep part of the EAC and with the chorda tympani nerve exposed (arrow). EAC indicates external auditory canal.
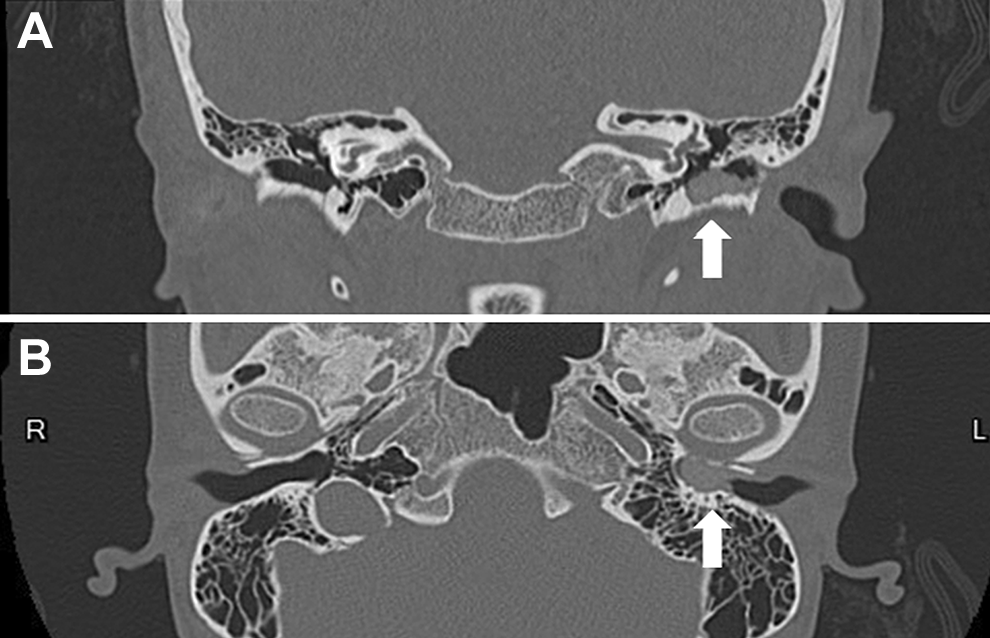
Coronal view (A) and axial view (B) of HRCT of the temporal bone indicated a nodule-like lesion with the size of approximately 0.6 × 0.6 × 1.2 cm3 in the left EAC, abutting the tympanic membrane with a widening EAC and bony erosion of the hypotympanum (arrow). EAC indicates external auditory canal; HRCT, high-resolution computed tomography.
Keratosis obturans is a rare disease characterized by abnormal accumulation with a dense plug of desquamated keratin, which causes an occlusion and expansion of the bony portion in the deep EAC. 1 The etiology of KO remains uncertain and should be differentiated from that of EAC cholesteatoma.2-4 The most common symptoms of KO in EAC include conductive hearing loss, severe otalgia, a widened ear canal without osteonecrosis or bony sequestration, and a thickened tympanic membrane, but otorrhea is rare.3,4
Acute neuropathy is relatively rare; this includes involvement of the facial nerve or its branch (the chorda tympani nerve) that is caused by KO in the deep part of the EAC. Glynn et al reported acute facial palsy secondary to a neglected KO. 3 Persaud et al described a case of KO in which the principal symptom was a metallic taste, and the operative finding was similar to that of our presented case. 5 We surmise this similarity to stem from the mass effect of KO—with an expansion of the EAC and compression of the chorda tympani nerve—in causing acute taste loss. 5 Our case illustrates an unpresenting symptom that may be a late complication of KO, thereby warranting early management to prevent severe complications.
Footnotes
Authors’ Note
Because the patient’s identity is not identifiable through the figures and the research content, a patient consent statement was not added.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-D-109053 to H. C. Chen).