
Abstract

A middle aged lady presented with left ear block and nonfoul smelling mucoid ear discharge of 2 months duration. Eight years earlier, she had undergone left cortical mastoidectomy with type 1 tympanoplasty and endoscopic sinus surgery for chronic otitis media (COM) and nasal polyposis, respectively. Her ear discharge recurred 3 months later.
On examination, her left ear showed a small central perforation in pars tensa with thick mucoid discharge. Baseline audiogram showed moderate conductive hearing loss on the left with normal hearing on right side.
A high resolution computerized tomography of the temporal bone showed an isointense opacification in the previous mastoidectomy cavity and middle ear. As the patient did not respond to antibiotics, she was planned for a revision mastoidectomy. Intraoperatively the mastoidectomy cavity was filled with pale granulations and viscous discharge. The disease in the tympanomastoid cavity was cleared and a temporalis fascia graft was used to close the perforation by underlay technique.
Histopathological analysis revealed inflammatory granulation tissue, acute inflammatory exudate, and eosinophilic micro abscesses suggestive of eosinophilic otitis media (EOM; Figures 1, 2, 3). There were no granulomas. Special stains for fungal microorganisms were negative. An immunoglobulin E (IgE) titer of 1783.3 further confirmed the diagnosis of EOM.
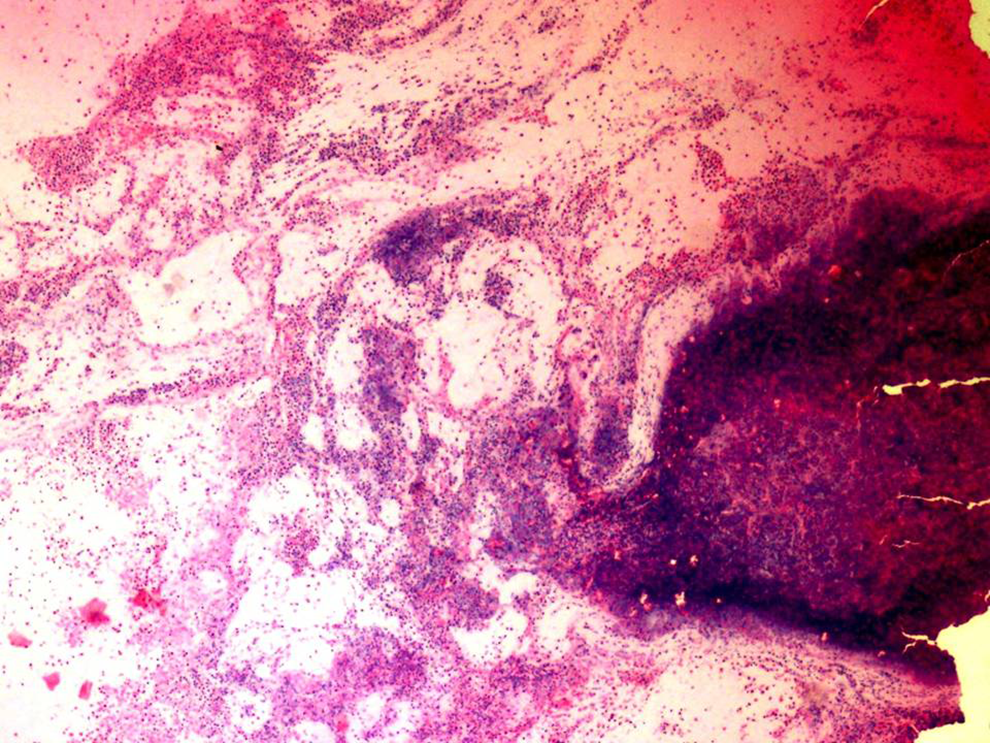
Hematoxylin and eosin stain, ×10, Acute inflammatory exudate.
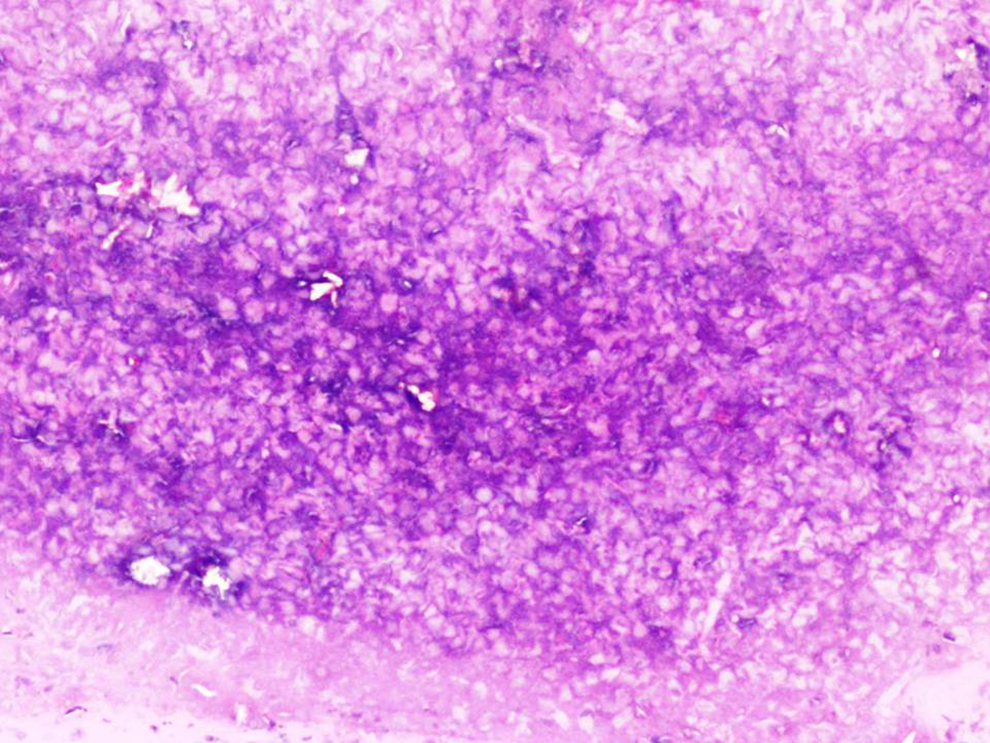
Periodic Acid Schiff stain, ×20, Acute exudate with nuclear debris and no fungal organisms.
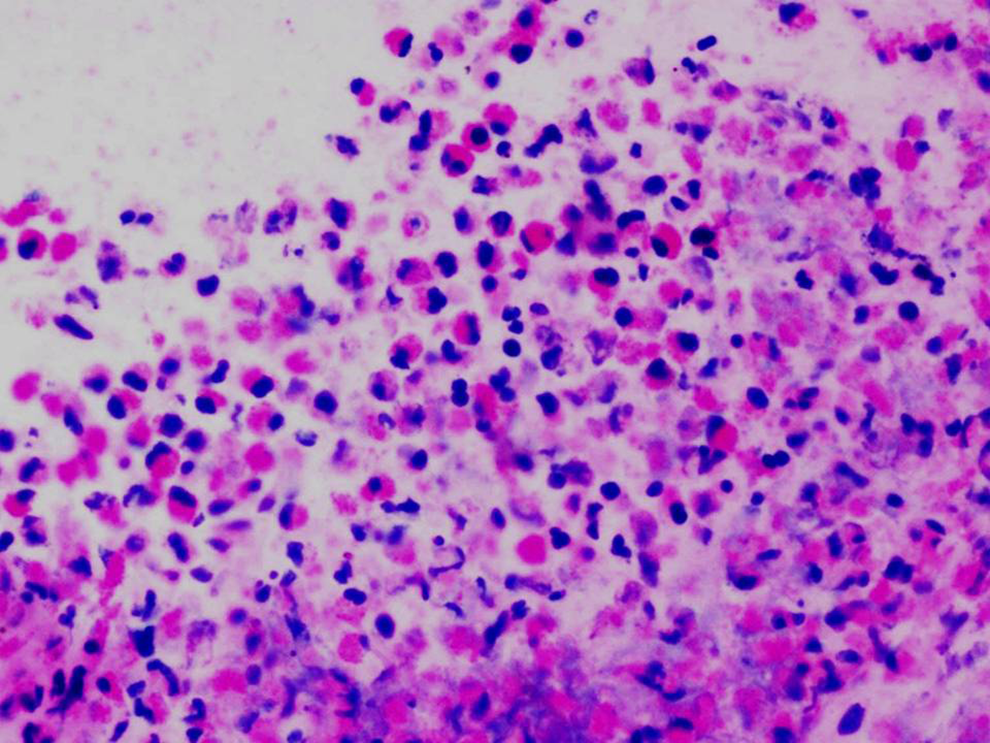
Hematoxylin and eosin stain, ×40, Acute inflammatory exudate containing neutrophils and numerous eosinophils forming microabscesses.
The patient returned with persistent ear discharge 3 weeks following surgery with a residual perforation and significant deterioration in hearing. In view of the histological features of EOM, she was subsequently treated with oral prednisolone for a month after which her ear discharge subsided.
Eosinophilic otitis media is a less identified type of otitis media often intractable to conventional treatment for COM. In 1997, Tomioka et al aptly coined the term based on the highly viscous middle ear effusion, rich in eosinophils with elevated levels of IgE. 1 The disease commonly affects women in their fifth decade. 2
The diagnostic criteria for EOM were put forward by EOM study group in Japan. 3 Major criterion: otitis media with effusion (OME) or COM with eosinophil dominant effusion. Minor criterion (2 or more among the following 4 items): (1) highly viscous middle ear effusion, (2) resistance to conventional treatment for otitis media, (3) association with bronchial asthma, (4) association with nasal polyposis.
Based on middle ear clinical features, Iino classified EOM into otitis media with effusion type and COM type. Chronic otitis media type is further subdivided into simple perforation and granulation tissue formation. 4
Histopathology is diagnostic with extensive accumulation of eosinophils and IgE immunopositive cells in middle ear mucosa. Edematous mucosa causing granulation tissue in the mesotympanum is considered a characteristic of EOM. 5 Esu et al has classified EOM into 3 grades based on the middle ear mucosal thickness where grade 1 (G1) is normal middle ear mucosa; grade 2 (G2), thickened mucosa localized to the middle ear; and grade 3 (G3), edematous mucosa with predominant granulation tissue extending to the external auditory canal. 6 The granulations are recalcitrant to conventional treatment for COM but show exceptional results with steroid therapy.
The middle ear effusion in EOM is rich in eosinophil cationic protein (ECP),7,8 interleukin-5 (IL-5), and eotaxin. The middle ear mucosa shows significant collection of EG2 (a monoclonal antibody to ECP) positive cells. Eosinophil cationic protein concentration has a positive correlation with IL-5, a cytokine actively involved in eosinophil migration, local activation, and increased survival of eosinophils leading to the underlying pathological eosinophilic inflammation in EOM. 7
Eosinophilic otitis media is associated with a significant risk of sudden or progressive hearing loss with unilateral or bilateral deafness reported in 5.8% patients. It is believed to be due to violation of inner ear by inflammatory products diffusing through the round window membrane. Adequate control of eosinophilic inflammation and superimposed bacterial infection is crucial in preserving residual hearing.
Systemic or topical glucocorticoids are considered very effective in managing EOM. This is in contrast to management of conventional OME or COM where treatment strategies include myringotomy, grommet insertion, antibiotics, or tympanomastoid surgeries. Many patients with EOM are often misdiagnosed and treated as COM, often with multiple unsuccessful revision surgeries.
Iwasaki et al speculated that mastoid surgery may promote accumulation of activated eosinophils thereby increasing the susceptibility of patients to chemical mediator induced inner ear damage and associated deafness 9 and suggested surgeries were to be avoided. A multi-institutional study showed a significantly higher ratio of deafness among patients who underwent tympanoplasty compared to those without tympanoplasty (17% vs 4%, P < .05). Hence it is imperative to have an accurate early diagnosis and initiate appropriate treatment to avoid unnecessary surgeries and consequences like permanent deafness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.