
Abstract
Arytenoid dislocation and subluxations commonly are reduced surgically using Holinger and straight Miller-3 laryngoscopes. We present a case of arytenoid cartilage subluxation returned to good position using a 28-Jackson dilator. A 66-year-old man was diagnosed previously with right vocal fold paresis and left vocal fold paralysis following a motor vehicle accident that required a 14-day intubation and tracheotomy maintained for 3 weeks. Evaluation by strobovideolaryngoscopy 3 months following the accident showed severe left vocal fold hypomotility and arytenoid height disparity; laryngeal electromyography showed only mild-to-moderate decreased recruitment in laryngeal muscles. No abnormalities were appreciated on neck computed tomography. Upon palpation of both arytenoid cartilages in the operating room, the left joint was found to be subluxed anteriorly and immobile. A 28-Jackson dilator was used to mobilize and reduce the left arytenoid cartilage, and steroid was injected into the cricothyroid joint. Increased mobility was obtained in the operating room and the patient reported significant improvement in his voice. Six months later, we saw improvement in arytenoid height disparity and left vocal fold movement, better glottic closure, and voice handicap index was improved. A 28-Jackson dilator can be used to manipulate the cricoarytenoid joint without trauma to the vocal process.
Introduction
Vocal fold hypomobility may be caused by paralysis, paresis, or arytenoid arthrodesis, dislocation or subluxation. Differentiating among these conditions is often complicated. Although early spontaneous reduction of arytenoid dislocation has been reported, 1 surgical reduction generally is required. Holinger and straight Miller-3 laryngoscopes have been used to return the arytenoid to improved or optimal position. This case of arytenoid anterior subluxation was reduced using a 28-Jackson dilator. The cricoarytenoid joint is diarthrodial with a fibrous capsule lined by synovium. 2 Cricoarytenoid joint dislocation has been implicated in partial airway obstruction and dysphonia. This report presents a patient misdiagnosed with left vocal fold paralysis and later found to have arytenoid subluxation. Arytenoid reduction was performed successfully using a 28-Jackson dilator 3 months after injury.
Case Presentation
The patient was a 66-year-old male former smoker and financial adviser with a chief complaint of hoarseness. He had been evaluated prior to our initial assessment by an otolaryngologist and diagnosed with right vocal fold paresis and left vocal fold paralysis. His problem began when he was in a motor vehicle accident that required hospital admission for 5 weeks. He had a concussion, multiple chest contusions, and rib fractures that were managed with orthopedic plates. He was intubated for 14 days followed by a tracheotomy. His tracheotomy was maintained for approximately 3 weeks, and he was decannulated before discharge. His voice handicap index (VHI) score was initially 16. Strobovideolaryngoscopy in our center 3 months after the accident initially revealed left vocal fold severe hypomotility and arytenoid height disparity (left was lower; Figure 1). Laryngeal electromyography (LEMG) showed only 30% to 40% decreased recruitment in the right thyroarytenoid and right posterior cricoarytenoid muscles, 20% to 30% decreased recruitment in the right cricothyroid muscle, 30% decreased recruitment in the left cricothyroid muscle, and normal recruitment in the remainder of the laryngeal muscles. The moderate left superior laryngeal nerve paresis was not severe enough to explain the severity of the hypomotility. No abnormalities were appreciated on neck computed tomography (CT).
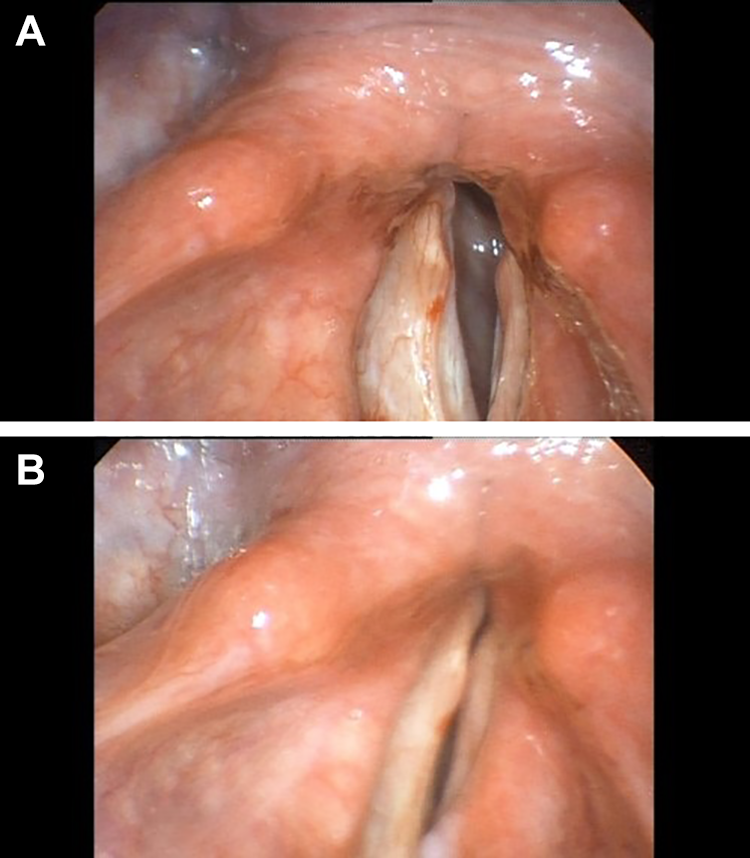
Arytenoid height disparity seen in abduction (A) and adduction (B).
The patient was taken to the operating room and both arytenoid cartilages were palpated. The left joint was found to be subluxed anteriorly and immobile. A 28-Jackson dilator (Figure 2) was used to mobilize and reduce the left arytenoid cartilage, and steroid was injected into the cricothyroid joint. Increased mobility was obtained. The patient reported significant improvement in his voice 4 weeks postoperatively. Strobovideolaryngoscopy postoperatively for 6 months showed sustained improvement in arytenoid height disparity and left vocal fold movement, better glottic closure (Figure 3), and his VHI improved to 10.

Size 28F Jackson laryngeal dilator (2020). Retrieved from https://www.teleflexsurgicalcatalog.com/pilling/product/507509-jackson-laryngeal-dilator.
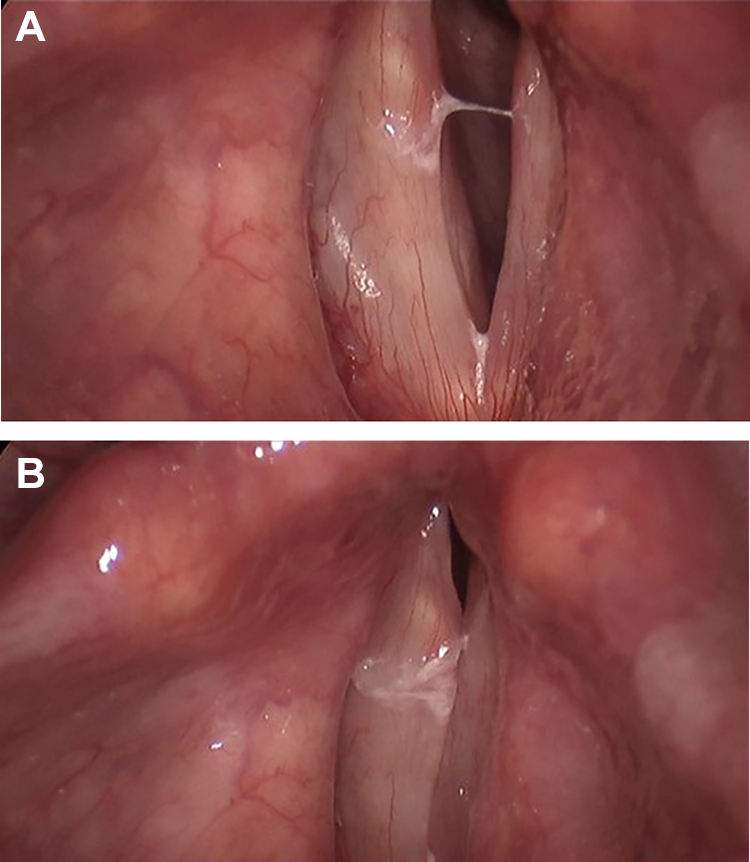
Arytenoid height disparity improved, but not corrected fully, seen in abduction (A) and adduction (B). In addition to vocal process height, glottic closure also improved.
Discussion
Arytenoid dislocation and subluxation (partial dislocation) commonly are related to intubation or laryngeal trauma. 2 They usually are suspected based on the history and absence of a jostle sign that is present in many cases of unilateral vocal fold paralysis. Often, arytenoid dislocation/subluxation is not diagnosed until direct laryngoscopy reveals impaired passive mobility of the vocal fold. Preoperative differentiation between vocal fold paralysis and arytenoid dislocation should be possible in virtually all cases. However, if not considered specifically, it often will be missed. The most valuable tests are the stroboscopic examination to visualize differences in vocal process height and presence or absence of Jostle sign; CT scan of the larynx, which sometimes images the arytenoid dislocation and reveals clouding or obliteration of the cricoarytenoid joint space; and LEMG to differentiate arytenoid joint dysfunction from vocal fold paralysis. 3 In this case, the patient had bilateral vocal fold mild-to-moderate paresis and left arytenoid subluxation which was seen easily on examination. The patient reported substantial improvement in his voice following closed reduction with intra-articular cricoarytenoid joint dexamethasone injection. The patient was followed for 6 months with a stable result.
Although anterior and posterior dislocations are described most commonly, 1 the arytenoids can be dislocated in any direction. The cartilage can be displaced partially (subluxation). In otolaryngology literature, the terms dislocation and subluxation have been used interchangeably; and most reported arytenoid dislocations are really subluxations. Reduction has been described previously using Holinger and Miller-3 laryngoscopes. The laryngeal dilator is of ideal shape and size to manipulate the cricoarytenoid joint with minimal trauma to the vocal process. The size 28F Jackson laryngeal dilators are rigid metal, 30 cm in length from tip to angle, with a triangular shaped end. They are manufactured by Teleflex in Morrisville, North Carolina. Although early reduction is optimal, a late reduction can be successful, and botulinum toxin may be useful as a chemical tenotomy to enhance results in cases of any duration.2,3 Intra-articular steroid injections can be effective in reducing inflammation and avoiding fibrosis in laryngeal manifestations of rheumatoid arthritis4,5 and we believe that injection might may be helpful following any arytenoid reduction. Although the goal of treatment is restoration of normal position and function, this cannot always be achieved especially in long-standing dislocation/subluxation cases.6–9 However, eliminating or improving vocal process height disparity often results in substantial voice improvement even if vocal fold motion is not restored.
Conclusion
Arytenoid subluxation is not rare. Conservative reduction using 28-Jackson dilator and steroid injections can be effective in selected cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.