
Abstract
The treatment of subglottic stenosis remains a challenge due to anatomic and technological limitations, and there is no consensus regarding treatment. Restenosis and granulation formation are the most common complications. Balloon dilatation combined with cryotherapy and adjuvant topical medication is one treatment method. However, the efficacy of adjuvant topical medication is controversial, and the lack of efficacy may be related to the effective dose of the drug delivered to the submucosal layer of the lesion. Therefore, a tool with high efficiency for delivering medications to the submucosal layer via injection may play an important role in treatment. A hybrid knife (HK) with a pressure water jet traditionally used in endoscopy submucosal dissection to inject saline into the submucosa was employed here to inject medications for subglottic stenosis, followed by electrical excision. Here, we report the case of a man with complex subglottic stenosis who underwent balloon dilatation combined with cryotherapy and an adjuvant submucosal triamcinolone injection performed with an HK. The drug was delivered more efficiently into the submucosal layer, and the lumen of the trachea was patent. Performing a submucosal injection with an HK may be a new approach to deliver medications to the submucosal layer for the treatment of tracheal stenosis.
Introduction
Subglottic stenosis (SGS) is caused by various reasons, and postintubation SGS is one of the most common causes. 1 The treatment of SGS remains a challenge due to anatomic factors and the occurrence of restenosis after treatment; however, various interventional bronchoscopic techniques have been used in the treatment of tracheal stenosis. 2 Therefore, it is crucial to prevent the recurrence of stenosis and scar formation. Balloon dilatation combined with cryotherapy and adjuvant topical medication to prevent the growth of granulation tissue is considered to be an appropriate treatment to prevent restenosis3-5; however, there are still some patients with unsatisfactory results related to the inadequate delivery of the medications to the submucosal layer of the lesion. Currently, medications are primarily delivered by local sprays and injections with needles; however, these approaches lead to a limited amount of drug remaining in the submucosal layer due to low permeability and low pressure. Therefore, a tool with high efficiency for delivering drugs to the submucosa via injection may play an important role in treatment. A hybrid knife (HK) is a diathermic knife with a pressure water jet and is mainly applied during endoscopic submucosal dissection (ESD) and pleural biopsy, in which the primary mechanism is submucosal lifting, incision, and dissection and coagulation.6,7 A HK may be a useful tool to incise the stenosis and deliver drugs to the submucosal layer of the lesion due to the use of a pressure water jet. Here, we report a patient with SGS who was successfully treated with a HK as an incision and drug delivery tool. The patient provided written informed consent to have the case report and accompanying images published.
Case Report
A 21-year-old male with an endotracheal tube for 3 years was admitted to our hospital in December 2017 and presented with a history of cough and shortness of breath for 1 month. He had a history of intubation for 5 days due to ingestion of pesticides in February 2014, but he did not exhibit SGS immediately after the intubation at the time of rescue. When referred to our hospital, the patient had complete obstruction due to the SGS and had a trach tube for 3 years after tracheotomy. The patient gave a disease history and information on the relationship of the SGS and intubation. Furthermore, he had no obvious gastroesophageal reflux syndrome during the 3 years. Thus, postintubation SGS was diagnosed. Tracheotomy, stenosis resection, and placement of a T-tube were performed sequentially, but restenosis occurred after treatment. Computed tomography (CT) of the chest and neck and bronchoscopy showed complete obstruction of the trachea, with stenosis located 1 cm below the glottis for a length of 4.0 cm (Figure 1A, B, C). The patient refused the attempt of surgical resection of tracheal stenosis. Bronchoscopic intervention was considered. We applied a needle for endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA; Olympus) to probe the distal trachea following cryotherapy (ERBOKRYO CA, ERBE Elektromedizin) after the guidewire failed (Figure 1 D, E, F, G, H). Then, balloon dilatation (CRE balloon M00550330; Boston Scientific) and cryotherapy were performed repeatedly. The VIO 300D generator (ERBE Elektromedizin) was used as a surgical system. A HK (ERBE Hybrid Knife ® I-type I-jet, ERBE Elektromedizin) was applied to make an incision in the stenotic area from the left to the right of the narrow segment (VIO mode ENDO CUT I, effect3-width1-interval of incision 4, Coagulation effect 2 and 30 W) followed by balloon dilatation to 8 mm (Figure 1I, J; Supplemental Digital Content, Supplement 1). However, the efficacy of balloon dilation and cryotherapy was limited, and restenosis occurred for the long length of the stenosis. Injection of topical medication combined with balloon dilatation and cryotherapy was considered. Triamcinolone (8 mg/mL, total dose 40 mg, Kunming Jida Pharmaceutical Co, LTD) was delivered to the submucosal layer of the stenotic area using the HK as a drug delivery system to prevent the occurrence of restenosis with 35 cm H2O of water jet pressure (Figure 1I; Supplemental Digital Content, Supplement 2). We performed only one incision at the initiation of treatment, and the medication was injected every 3 times for totally 3 times. Finally, the patient was successfully decannulated, with no obvious growth of granulation tissue and a patent tracheal lumen (Figure 1K, L).
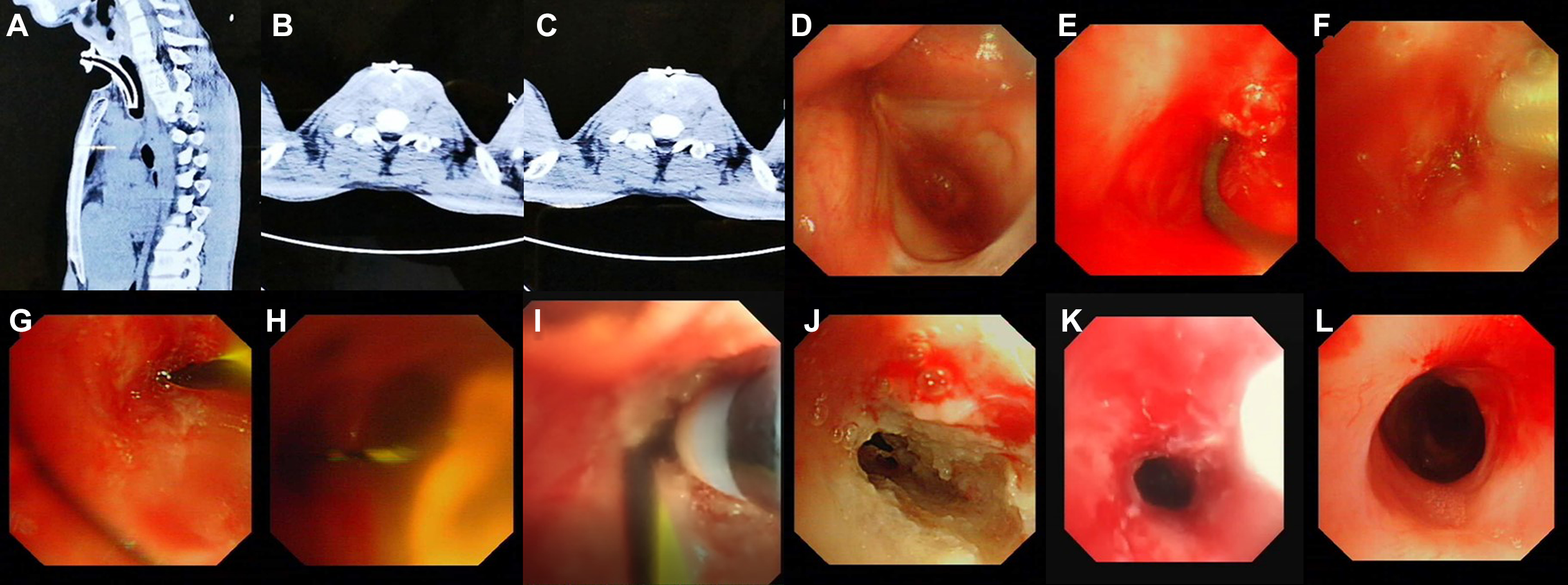
The manifestation on chest computed tomography and bronchoscopy. A, Sagittal view of chest computed tomography: the length of subglottic stenosis was 3 cm. B, The cross-section of the trachea showed that the lumen was completely obstructed. C, A small air space was seen at the left side of the tracheal lumen. This was the reason why we applied a needle for endobronchial ultrasound-guided transbronchial needle aspiration to probe the distal trachea via the left side. D, Bronchoscopy showed the subglottic stenosis. E, The guidewire could not find a space to pass through the obstruction. F, We applied a needle for endobronchial ultrasound-guided transbronchial needle aspiration to probe the distal trachea. G, We inserted the guidewire into the channel made by EBUS-TBNA needle puncture. H, We confirmed that the guidewire entered the distal trachea successfully. I, The guidewire was set as the marker of the start of incision with the hybrid knife. J, The subglottic stenosis was incised successfully. K, Because the restenosis occurred after repeated balloon dilation and cryotherapy, we used a hybrid knife to deliver triamcinolone into the submucosal layer of the stenotic segment. L, After 3 injections of triamcinolone with the hybrid knife, the patient was successfully decannulated, no obvious growth of granulation tissue was observed, and the tracheal lumen was patent.
Discussion
Postintubation tracheal stenosis remains a clinical challenge; even the application of low-pressure, high-volume cuffs can reduce the risk. The severity of tracheal stenosis mainly depends on the location, length, and extent of stenosis, and according to these factors, a suitable therapeutic strategy is chosen. Currently, surgical treatment has been advocated as the treatment of choice, with success rates reported from 84% to 100% after 1 month to 12 years of follow-up. 8 Currently, tracheal transplant or reconstruction surgery is also considered. 9 Surgical reconstruction of the trachea is contraindicated for some patients with long, narrow segments, and some patients refuse the surgical treatment due to potential complications. Endobronchial treatments may be offered as a bridge to surgery or when surgical treatment is not possible due to the extent of the lesion or patient factors. Bronchoscopic intervention was an alternative for patients with tracheal stenosis.
However, the restenosis and granulation tissue formation are the most commonly reported complications after bronchoscopic interventional treatment, including balloon dilatation, electrosurgery, laser, and T-tube or stent implantation. Local drug injection has been considered an effective therapy to prevent the growth of granulation tissue and prevent restenosis. However, the efficacy of drug injection remains controversial. 10 Some studies have indicated that steroids have no effect in preventing SGS. 11 In contrast, other studies have suggested that the use of local steroid injection can prevent the formation of granulation tissue and restenosis. 12 A clinical study indicated that intralesional steroid injection combined with conventional interventional treatment could significantly decrease the rate of airway narrowing and increase the duration until restenosis compared with conventional interventions alone. 4 The inconsistent effect of steroid therapy may be related to the effective dose delivered into the submucosa of the stenotic segment.
Transcervical injection and transnasal injection with flexible needles are common methods of injecting steroids; however, fibrosis is mainly located in the basal layer of the trachea in patients with SGS, and drugs delivered by conventional injection needles cannot effectively penetrate this area due to the low pressure of injection. A HK with a high-pressure water jet applied during ESD as a tool for submucosal injection can allow more of the injected drug to remain in the basal layer and has improved efficacy of drug injection.
Various steroids have been applied, and triamcinolone is commonly used. Triamcinolone, a synthetic long-acting steroid with strong and effective anti-inflammatory and antiallergic effects, can be locally injected into the submucosa to inhibit the formation of granulation tissue and delay restenosis.5,13 In this case, we applied balloon dilatation and cryotherapy with an adjuvant injection of triamcinolone with a HK, and the results showed that local triamcinolone injection administered with a HK was effective. In addition, in this case, we also applied a HK to make an incision in the stenotic area from the left to right of the narrow segment with a guidewire after determining the shape of the narrow segment on CT; this technique may exhibit better efficacy than that of treatment with an electrosurgery knife due to the length and stiffness of the HK tip.
However, there are several limitations of this report. We reported only one case, and more cases of tracheal stenosis should be evaluated. Furthermore, a randomized controlled trial comparing the efficacy of using a HK with a traditional injection needle is needed to demonstrate the safety and efficacy of using a HK as a drug delivery tool. In addition, long-term follow-up should be performed for these patients to observe the long-term treatment efficacy.
Conclusion
In summary, a HK, a diathermic knife with a high-pressure water jet, is a potentially useful tool for incision and drug injection for the treatment of tracheal stenosis, especially for patients with a long segment of stenosis and restenosis after recanalization.
Supplemental Material
Supplemental Material, sj-jpg-1-ear-10.1177_0145561320946649 - Hybrid Knife, a Novel Drug Delivery Tool for Treatment of Tracheal Stenosis: A Case Report
Supplemental Material, sj-jpg-1-ear-10.1177_0145561320946649 for Hybrid Knife, a Novel Drug Delivery Tool for Treatment of Tracheal Stenosis: A Case Report by Yan Yin, Wen-hui Ma, Wei Li, Hai-feng Ma, Jian Kang, Felix J. F. Herth and Gang Hou in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
G.H. substantially contributed to the conception or design of the work. Y.Y., G.H., W.-H.M., W.L., and H.-F.M. contributed to acquisition of data for the work. G.H., F. J. F. H., and J.K. contributed to analysis and interpretation of data for the work. F. J. F. H. and G.H. contributed to revising the manuscript critically for important intellectual content. All authors contributed to drafting the manuscript, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.