
Abstract
A 72-year-old male patient with painless, round, tight elastic consistency mass at the side of the bifurcation of the common carotid artery was selected for carotid body tumor (CBT) excision with intraoperative intratumoral injection of gelatin–thrombin matrix (III-GTHM). Magnetic resonance imaging confirmed the hypervascularized 4.5 cm × 3.5 cm × 2.5 cm in diameter mass in the carotid bifurcation, with low signal intensity on T1-weighted imaging and heterogeneous signal intensity on T2-weighted imaging (Figure 1). Intense diffuse enhancement occurred after intravenous administration of gadolinium. The mass was splaying and displacing of the internal and external carotid arteries (Lyre sign). Preoperatively, a detailed angiography was performed. The superselective embolization was done 1 day before the surgery. Informed consent was obtained from the patient to publish his details and images. Gelatin–thrombin matrix is injected into the center, superior, anterior, posterior, and inferior part of the tumor (Figure 2). It is not injected too close to the external carotid artery, bifurcation, and the internal carotid artery to avoid the possible thrombotic effects. Gelatin–thrombin matrix of 10 cc was injected into the tumor. Wait time of 10 minutes is required for performing the hemostasis in the tumor vasculature using GTHM (Supplement video).
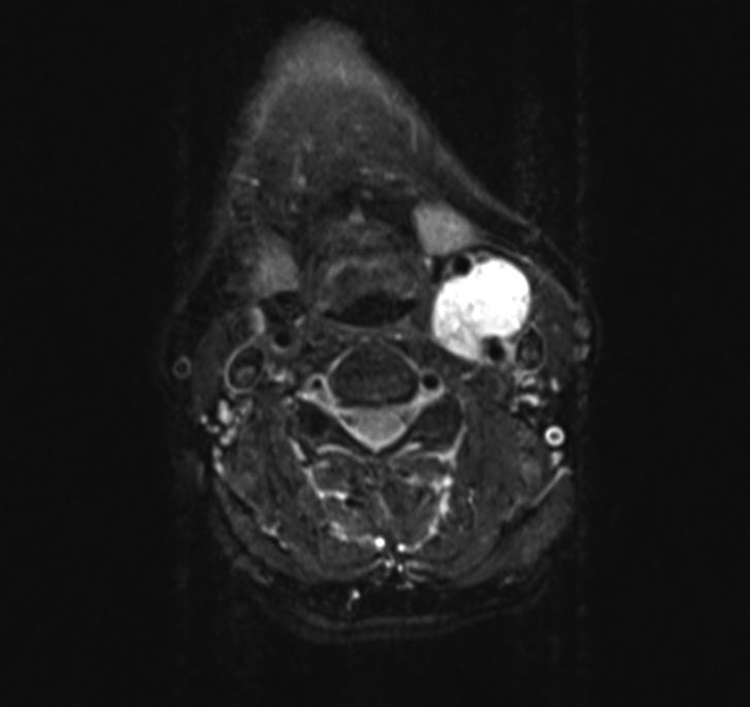
Neck magnetic resonance imaging T2-weighted, axial plane, hypervascular 4.5 × 3.5 × 2.5 cm in diameter mass at the level of bifurcation.
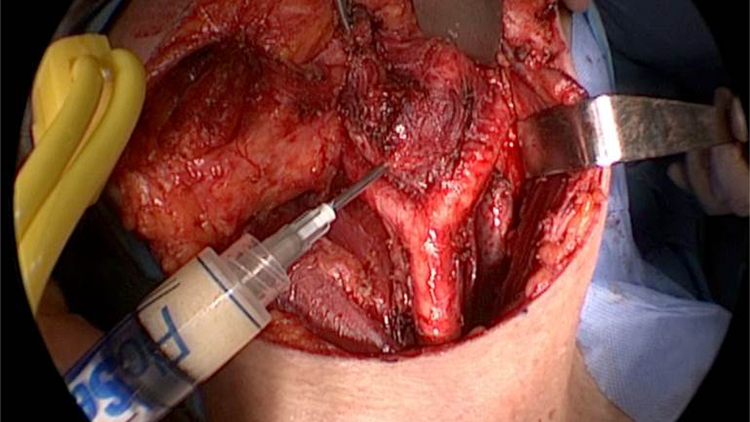
Intraoperative intratumoral injection of gelatin–thrombin hemostatic matrix.
Carotid body tumor is the most common form of cervical paraganglioma. Approximately 90% of CBTs are sporadic and 10% are familial. 1 Carotid body tumors are commonly seen in the fourth to sixth decades of life. These highly vascular mostly benign neoplasms are rarely functional (1%-3%). 1 The primary therapeutic goal for CBT is complete tumor excision with preservation of the neurovascular structure. Although there is improvement in surgical treatment, complications continue to occur. Devascularization of the tumor has become an important adjunct to surgery, as it facilitates the total surgical removal of these tumors and minimizes morbidity consequent to blood loss and bloody surgical field.2-4 Superselective catheterization, transarterial embolization, direct percutaneous intratumoral injection, and stent placement techniques are used for minimizing the intraoperative bleeding. Because of the angioarchitecture characteristics of the tumor, complete devascularization of the tumor is rarely achieved. During the peeling of surrounding fascia for freed tetrad, there was 85 cc bleeding although we use bipolar diathermy and the tumor was embolized preoperatively. But, after the III-GTHM injection, dissection of the tumor from the internal carotid artery and external carotid artery and bifurcation in the subadventitial plane were done with scissors easily. During the cold dissection, almost no bleeding was seen and mass dissection was done within 5 minutes.
Power et al showed that the estimated bleeding amount decreased from 410 to 263 cc. 5 With the use of III-GTHM, mean blood loss was reduced to 85 cc. Although preoperative embolization is extremely important in reducing the mean estimated blood loss, 5 this amount will be further reduced by adding intraoperative intraoperative injection of GTHM to embolization. After tumor excision, we bisected the tumor. We observed that the vascular channels were obstructed by III-GTHM, which explains our technique success.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.