
Abstract

A 59-year-old woman was referred to our clinic for a mass on the right epiglottis that was found incidentally. She had no history of drinking alcohol or smoking. She had a history of hypertension and was diagnosed with diabetes during preoperative evaluation. Flexible endoscopy revealed an exophytic, irregular mass involving the laryngeal surface of the right side of the epiglottis. Computed tomography demonstrated a 1.9 × 0.9 cm irregular, gradually enhancing lesion on the right laryngeal surface of the suprahyoid and infrahyoid epiglottis (Figure 1). To rule out supraglottic cancer, we performed direct laryngoscopy and biopsy. Direct laryngoscopy revealed a bulky, irregular, firm supraglottic mass arising from the epiglottis (Figure 2). Histopathological examination of the frozen section revealed squamous epithelial hyperplasia with an endophytic growth pattern. Final histopathological examination of the additional tissue biopsy revealed squamous epithelial hyperplasia covered by ciliated columnar cells showing inverted growth and stromal lymphoid follicles, most likely indicative of inverted papilloma (IP). The patient was rehospitalized for total resection of the IP. During surgery under general anesthesia, the mass was exposed sufficiently and seen to cross the midline of the epiglottis. About two-thirds of the epiglottis, including the mass, was resected en bloc using a CO2 laser in 3-watt continuous mode. The resection margin of the surgical specimen was free from the tumor. Histopathological examination revealed an IP with inverted growth and epithelial islands with distinct and continuous basement membranes, hyperplastic nonkeratinizing squamous epithelium, and innermost respiratory ciliated columnar cells with scattered mixed inflammatory cells (Figure 3). On the day after partial epiglottectomy, she started eating a special diet to prevent aspiration using a supraglottic swallowing maneuver. A week after the operation, the patient was discharged without any postoperative complications. The patient has been followed up for 1 year and 3 months, and no evidence of recurrence has been observed.
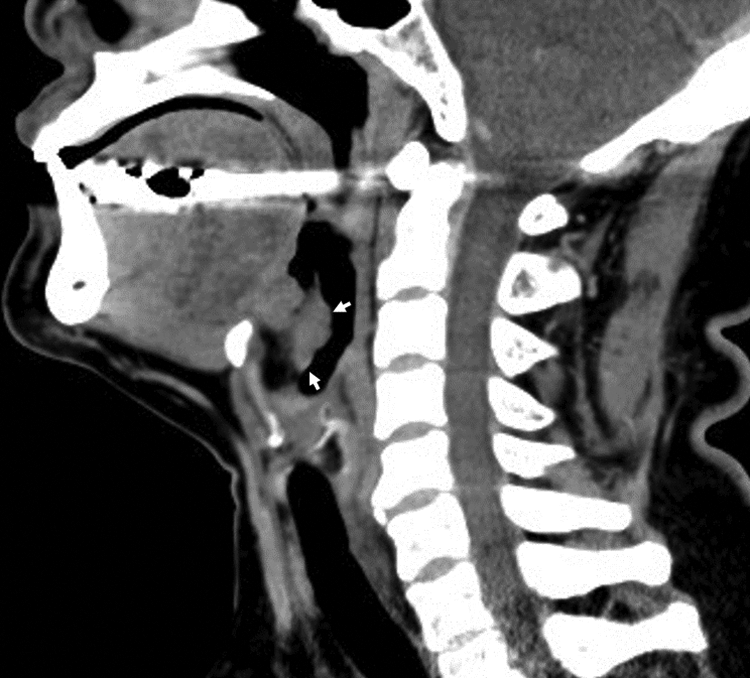
Sagittal contrast-enhanced computed tomography shows an irregular, gradually enhancing lesion on the laryngeal surface of the suprahyoid and infrahyoid epiglottis (arrow).

Direct laryngoscopy shows a bulky, irregular, firm supraglottic mass arising from the epiglottis.

Histopathological findings. (A) Inverted growth and the epithelial islands with distinct and continuous basement membrane (H&E stain, ×40). (B) Hyperplastic nonkeratinizing squamous epithelium and innermost respiratory ciliated columnar cells with scattered mixed inflammatory cells (H&E stain, ×100).
Sinonasal papilloma is a benign neoplasm originating from the Schneiderian membrane, which is the ectodermally derived mucosa that lines the nasal cavity and paranasal sinuses.1,2 According to the World Health Organization classification, Schneiderian papilloma can be divided into 3 types: inverted, exophytic, and oncocytic papilloma. 3 Inverted papilloma has the histological appearance of the epithelium inverting into the stroma, with a distinct and intact basement membrane that separates and defines the epithelial component from the underlying connective tissue stroma. 4 Inverted papilloma occurs most commonly on the lateral nasal wall and middle meatus and extends to the contiguous paranasal sinus. 1 To date, ectopic occurrence of IP arising from the outside the sinonasal tract has been reported in the nasopharynx, oropharynx, middle ear, mastoid, temporal bone, supraglottis, subglottis, and lacrimal sac.2,5-10 However, IP involving the larynx as a primary lesion is extremely rare. To the best of our knowledge, there are only 2 cases of IP arising from the larynx reported in the English literature.8,9 The exact etiology of IP is not known. Although the etiology of sinonasal IP remains controversial, human papilloma virus, smoking, industrial exposures, cell cycle–related proteins, angiogenic factors, and chronic inflammation have been suggested. 11 In IP involving the middle ear, direct extension or migration of tumor cells from the sinonasal IP via the Eustachian tube, embryonic migration of ectopic Schneiderian epithelium into the middle ear mucosa, and chronic inflammation related to chronic suppurative otitis media have been hypothesized. 6 The reported patient with supraglottic IP had a history of regular smoking and intermittent gastroesophageal reflux events; the chronic inflammation that is a likely consequence of gastric reflux and smoking is a plausible explanation for laryngeal IP. 8 In the case of subglottic IP, no suspected cause was found in a 4-year-old boy. 9 The patient of our case was a healthy adult with no past history except for hypertension and diabetes; it is not possible to identify the cause of supraglottic IP and which hypothesis played a crucial role in our case.
Inverted papilloma is benign but has a tendency for recurrence and potential for malignant transformation. The recurrence rate and malignant transformation for sinonasal IP ranged from 14.3% to 34.9% and 9% to 13.64%, respectively.1,12 The major cause of recurrence of IP is incomplete resection of the lesion. 13 For sinonasal IP, the treatment of choice is complete surgical resection. 14 Similarly, transoral laser microsurgery can be an option for complete resection of laryngeal IP without external approaches. Preoperative laryngoscopy and imaging studies are essential to plan the extent of surgery and surgical methods. Long-term follow-up is needed to detect any possible recurrence or metachronous malignancy of laryngeal IP early.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article