
Abstract

A 58-year-old homeless male was brought to emergency department with altered mental status, lethargy, right ear pain, and right ear discharge for the past few days. His past medical history was significant for acquired immunodeficiency syndrome (AIDS) noncompliant with antiretroviral therapy, chronic hepatitis C, chronic kidney disease, and polysubstance abuse especially snorting cocaine. On physical examination, the patient appeared cachectic, in no acute distress. There was tenderness to palpation over the right periauricular area with a visible abscess measured 2 cm × 3 cm just anterior to the tragus, grossly visible right nasal perforation measuring 1 cm × 1 cm (Figure 1). Ear, nose, and throat evaluation showed right otorrhea, intact right tympanic membrane, opaque, anterior canal wall erythematous with significant prolapse of the right temporomandibular joint (TMJ) into canal, there was pain with palpation of right TMJ, left external auditory canal was occluded by cerumen. The rest of the physical examination was not contributory.

Grossly visible right nasal perforation measuring 1 cm × 1 cm.
An initial noncontrast computed tomography scan of the head showed possible right mastoiditis and TMJ osteomyelitis (OM) (Figure 2). Magnetic resonance imaging of the head without contrast confirmed these findings along with OM involving the mandibular condyle and septic arthritis of the TMJ (Figure 3).

Head computed tomography (CT) without contrast showing possible right mastoiditis and TMJ osteomyelitis.
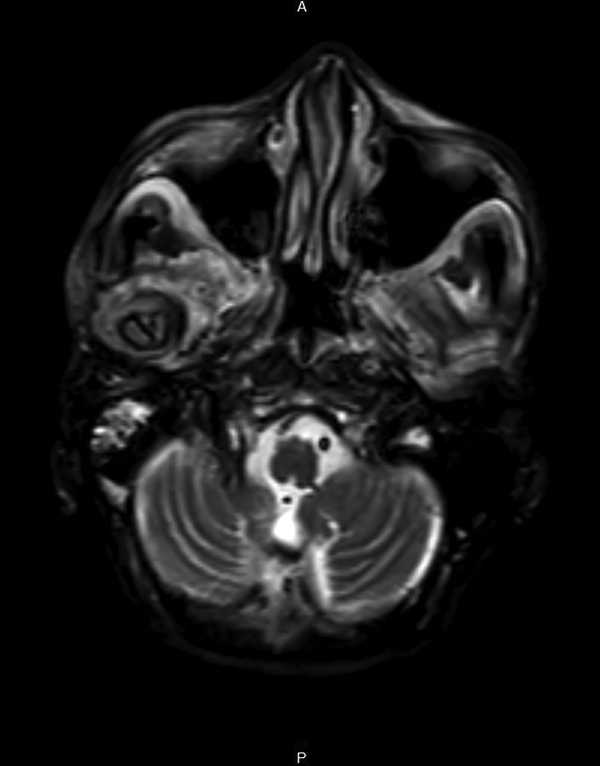
Magnetic resonance imaging (MRI) of the head without contrast confirmed these findings along with OM involving the mandibular condyle and septic arthritis of the TMJ. OM indicates osteomyelitis.
Blood and right ear drainage fluid cultures grew methicillin-sensitive Staphylococcus aureus. The patient was placed on intravenous nafcillin 2 gram every 4 hours. Transesophageal echocardiogram did not reveal any vegetation on the cardiac valves.
The patient underwent incision and drainage of the right infected TMJ, arthrotomy, and a biopsy of the mandibular right condyle. During the procedure, pus was noted in the right TMJ space, the right condyle was partially eroded, debris was removed and the joint space was thoroughly irrigated. Bone biopsy pathology showed limited fragments of bone with marrow fibrosis and spindle cells without acute inflammation. Bone biopsy culture isolated rare growth of Candida glabrata after 2 weeks thought to be a contaminant.
On the 3rd week of the admission, patient experienced a cardiac arrest and expired.
Temporomandibular joint OM is uncommonly encountered entity; it is estimated to be 1.5% of all cases of all OM. 1 Temporomandibular joint septic arthritis is mainly seen in patients with malignant otitis externa where infection may rarely progress to involve the surrounding bone leading to TMJ OM. 2 Temporomandibular joint infections can also be caused by contiguous spread from periauricular, odontogenic or masticator infections. 3 Staphylococcus aureus and Streptococci are the leading causes of TMJ septic arthritis 1 ; however, TMJ OM is most commonly caused by Pseudomonas aeruginosa and rarely by fungal pathogens like Candida and Aspergillus species especially in immunocompromised patients. 4 Hematogenous spread to the TMJ was described in some cases with Streptococci being the implicated organism. 5 Rhodococcus equi was reported as the cause of TMJ septic arthritis in an AIDS patient who presented with severe otitis and mastoiditis. 6
Temporomandibular joint OM has a mortality rate of 30% to 60% especially if the diagnosis and treatment are delayed. 2 Clinically patients present with swelling, tenderness, erythema, or unilateral facial pain. Risk factors for development of TMJ OM include diabetes mellitus and immunosuppression. 2
Mandibular condyle OM has been rarely reported, Bacteroides species, Staphylococcus species, group C Streptococcus, and Acinetobacter baumannii were reported as causative organisms.3,7
Our case is unique, the patient had AIDS and presented with a perforated septum due to cocaine use, this raises the possibility that the causative agent penetrated from the nasal area to cause a chronic Staphylococcal infection. To our knowledge this case represents the first case of TMJ OM with involvement of the mandibular condyle, caused by Staphylococcus aureus, in a patient with AIDS.
Footnotes
Authors’ Note
This article was not previously presented or published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.