
Abstract

Introduction
The petrous apex is an important part of the skull base and is intimately related to many important structures. Many different lesions are seen here in children—both benign and malignant. Cholesterol granulomas are the commonest petrous apex lesions in adults but are rarely seen in children. They are treated surgically when they cause symptoms. Various approaches have been described in the literature—both open and endonasal endoscopic. In this case report, we used an endonasal transsphenoidal approach that was selected based on audiology and imaging.
Patient Presentation
A 12-year-old boy presented to us with a history of blurring of vision for 4 months. On examination, he was found to have a left abducent nerve palsy. The rest of his clinical and ENT examination was unremarkable. His hearing was intact. Magnetic resonance imaging (MRI) of the brain showed a left petrous apex mass 1.8 cm × 1.2 cm × 9.8 cm in diameter eroding the left clivus. The mass was hyperintense on T1- and T2-weighted MRI. A diagnosis of cholesterol granuloma with a differential of Langerhans cell histiocytosis was made. The decision to operate was made based on the presence of a cranial nerve palsy and a destructive lesion on the left clivus (Figures 1 and 2).
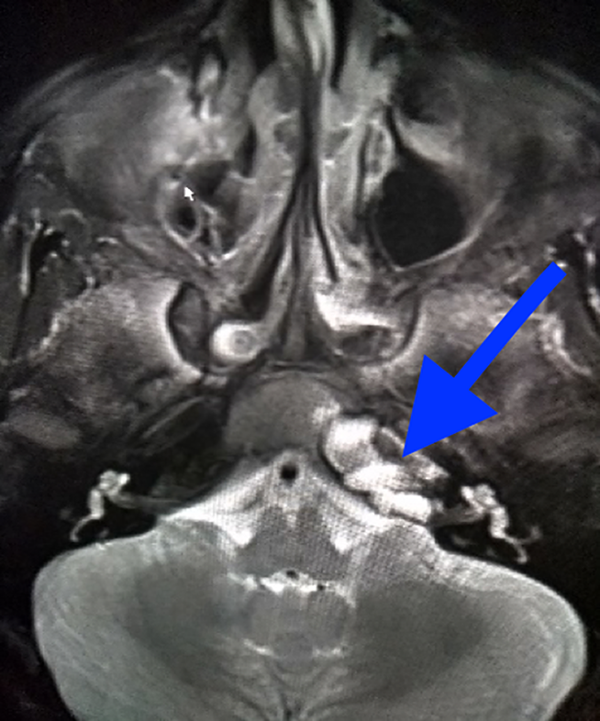
Magnetic resonance imaging hyperintense T1-weighted left petrous apex mass (blue arrow).
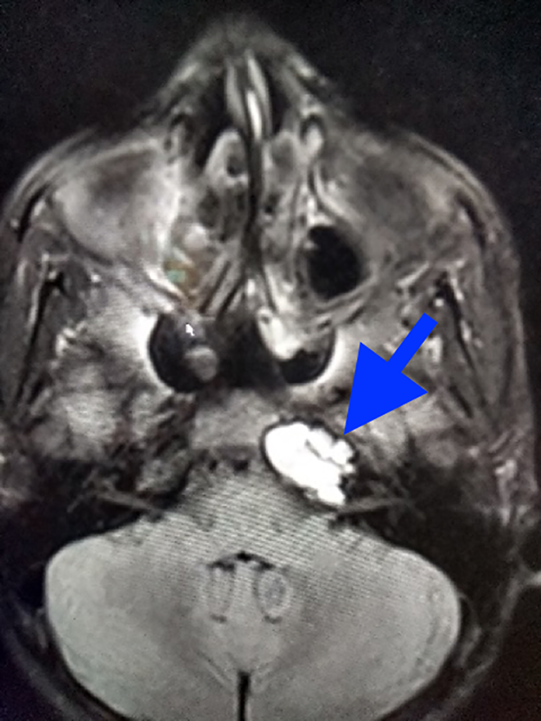
Magnetic resonance imaging hyperintense T2-weighted left petrous apex mass (blue arrow).
Management and Outcome
A transsphenoidal deroofing of the petrous apex cyst was done. The sphenoid sinus was breeched and the posterior wall was drilled into the left petrous apex under navigation. The cyst was drilled open and a small amount of dark fluid drained out (Figure 3). A small part of the cyst wall was biopsied. Due to its proximity to the carotid canal, only a small piece could be taken. The patient did not have any complications postoperatively and monitored in the ward. He was discharged on the third postoperative day.
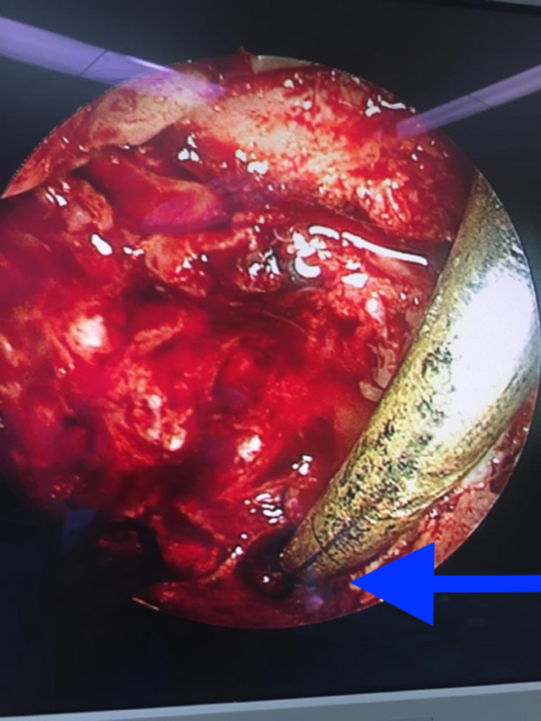
Petrous apex mass deroofed and drainage created into the sphenoid sinus (blue arrow).
On follow-up endoscopy, polypoidal changes were noted in the sphenoid sinus. The exteriorized cyst could not be visualized. Histopathology of the fragment of the cyst showed chronic inflammation and was too small for a conclusive diagnosis. The abducent nerve palsy and the blurring of vision resolved completely.
Discussion
Cholesterol granulomas are the commonest petrous apex lesions seen in the adult population. The incidence has been calculated to be 0.6 per 1 million population. The other lesions seen in the petrous apex are effusions and asymmetric pneumatization. These have been characterized as “leave-me-alone” lesions. Cholesterol granulomas in the petrous apex are extremely rare in the pediatric age-group especially before adolescence. 1
There are 2 main hypothesis for the development of cholesterol granulomas. Negative pressure due to Eustachian tube dysfunction causes bleeding into the petrous apex. This further incites a foreign body reaction and an inflammatory process resulting in the formation of a cholesterol granuloma. The other exposed marrow hypothesis postulates that there is an osseous dehiscence between the marrow of the petrous apex and the pneumatized air cells. When bleeding occurs into the air cell, the blood incites the same foreign body reaction and a cholesterol granuloma is formed.2,3
Due to the many important structures that are intimately related to the petrous apex, the clinical presentation of a petrous apex granuloma can vary. Patients can present with headaches, blurred vision, cranial nerve pathologies, hearing loss, or dizziness. Double vision or blurred vision is usually due to the compression of the sixth nerve in the Dorello canal.4,5
Radiographic studies are the single most important investigation for cholesterol granulomas. The investigation of choice is the MRI with contrast. Cholesterol granulomas are hyperintense without gadolinium contrast in T1-weighted images. In T2-weighted images, they are hyperintense.
The audiogram is critically important in selecting the surgical approach to the lesion. In this case, as the hearing was preserved, the anterior transnasal endoscopic approach was selected. 6
Conclusion
Petrous apex lesions can be managed successfully via endoscopic approaches (transsphenoidal, transclival, and transpterygoid). In this case, the transsphenoidal endonasal approach was successful in treating this patient. The endonasal approach has far fewer complications than the open approach. A recent comparative meta-analysis for the surgical management of cholesterol granulomas showed that the complication rate for the endonasal approach is 7.9% and for the open approach is 17.9%. The recovery period is also far shorter with no intensive care unit stay. 6
Endonasal approaches should be considered in managing pediatric petrous apex lesions. Adequate training and image guidance can make this a safe approach.
Footnotes
Authors’ Note
As the patients personal details were kept anonymous and no patient images were used, the Helsinki ethical principles were followed.
Acknowledgments
The authors would like to thank Dr Chris Quitter for his assistance during the surgical procedure.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.