
Abstract
Gastric signet ring cell carcinoma has well-known metastatic features, including peritoneal dissemination and carcinomatous lymphangitis of the lung, but no intraorbital metastases were reported previously. A woman in her 60s developed left eye pain, sudden vision loss, and headache 12 years after gastric cancer treatment. Symptoms did not improve despite steroid pulses. Craniotomy showed no malignant findings. The patient was referred to our department for symptomatic relief and biopsy due to the lack of a definitive diagnosis and no improvement in her ocular pain. Endonasal endoscopic surgery was performed for diagnostic purposes and to relieve symptoms through orbital decompression. Preoperative computed tomography examination revealed a tumor at the left medial orbit, extending to the orbital apex. Orbital decompression through the open left medial orbital wall was performed with biopsy of the intraorbital tumor. Pathological findings were consistent with metastatic signet ring cell carcinoma. Pain and subjective improvement of visual acuity were noted the day after surgery. Twelve months postoperatively, diplopia remains, but there has been no worsening of symptoms.
Keywords
Introduction
Metastatic gastric signet ring cell carcinoma (SRCC) is characterized by peritoneal dissemination and carcinomatous lymphangitis of the lung, but there has been only one report of intraorbital metastasis. 1 In this case, endonasal endoscopic orbial biopsy and medial orbital decompression was performed for orbital metastasis of SRCC, resulting in reduced ocular pain and visual impairment.
Case Report
A woman in her 60s presented to the ophthalmologist with pain, diplopia, and vision loss in her left eye for a year. She had undergone surgery for gastric SRCC 14 years ago and was followed up for 10 years without recurrence. Computed tomography (CT) revealed a tumor in the left orbit. As intravenous corticosteroids did not relieve symptoms, craniotomy was performed by a neurosurgeon for biopsy and decompression; however, this did not relieve the pain. Pathological examination of the biopsy sample demonstrated acidophilic fibrous tissue.
A CT examination during the hospitalization for craniotomy revealed a tumor in the mammary gland. Biopsy revealed SRCC and partial mastectomy was performed. Postoperative pathology showed metastasis of gastric SRCC. The patient was then referred to our department for definitive diagnosis of the left intraorbital tumor and symptom palliation.
She presented with left orbital pain, superior and hypertropia, visual impairment (visual acuity 0.06, unmeasurable critical flicker frequency value), and ocular protrusion. Endoscopy showed no abnormal findings in the left nasal area. Sinus CT showed a low-density, soft-tissue mass extending from the lateral side of the eye to the orbital apex on the medial side of the left orbit (Figure 1A and B). Magnetic resonance imaging revealed diffuse T1 and T2 low-intensity lesions in the same area (Figure 1C and D).
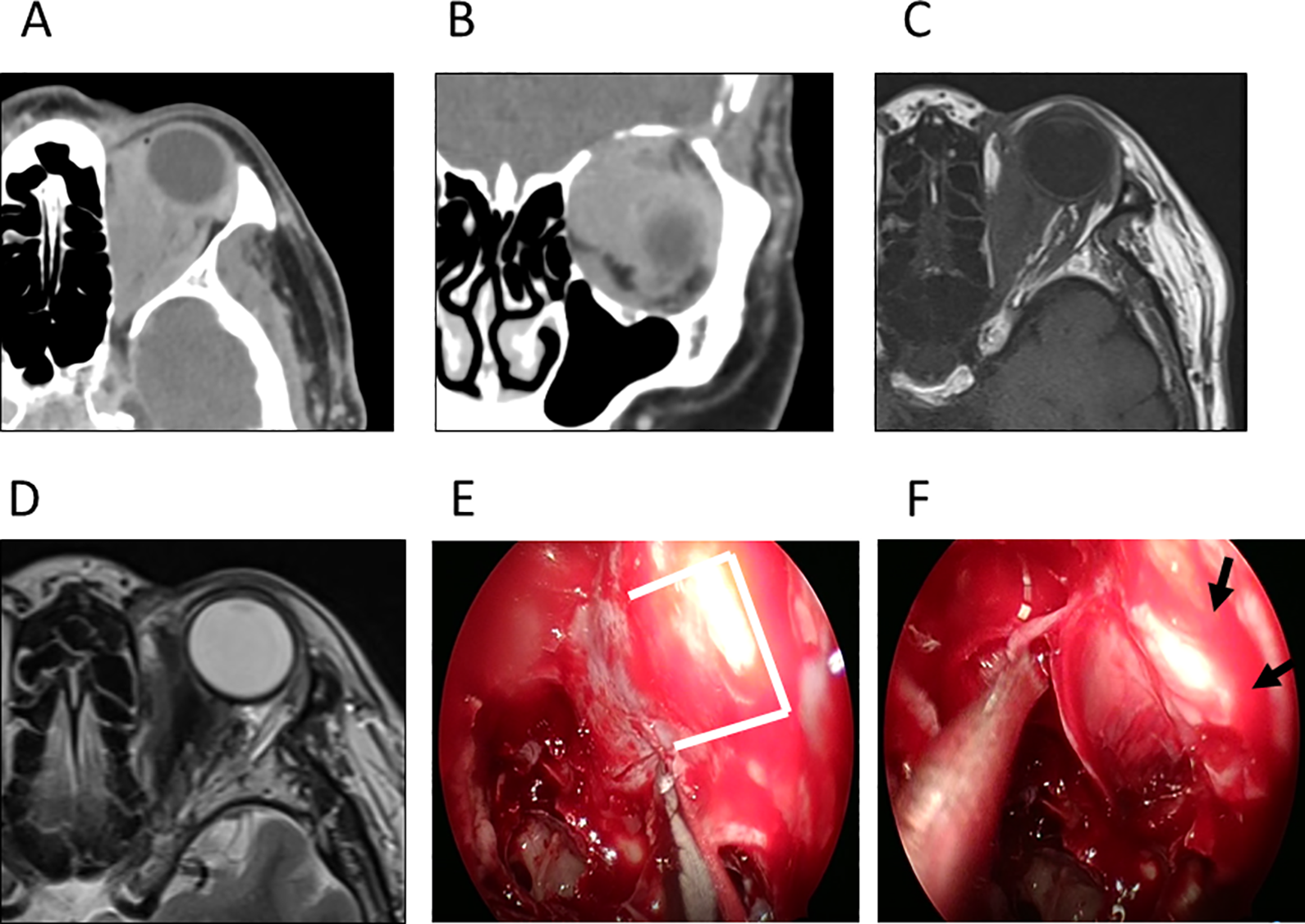
Preoperative sinus computed tomography (CT), magnetic resonance imaging (MRI), and intraoperative images. Preoperative sinus CT (A: axial transect, B: coronal transect): left orbital medial with a low-density, soft-tissue mass extending from the posterior part of the eye to the orbital apex (arrow), but no bony destruction of the orbital medial wall. Sinus MRI (C: T1-weighted image, D: T2-weighted image): Diffuse T1 and T2 low-intensity lesions were found in the same area as the lesion observed on CT (arrow). Intraoperative Images: (E: After identifying the medial orbital wall, the lamina papyracea was removed and the periosteum was incised. F: White, suspicious lesions were noted. Removal of the periosteum resulted in protrusion of the tumor into the sinuses and successful decompression. This was followed by tumor biopsy.)
Endoscopic surgery was performed under general anesthesia for the purpose of biopsy and orbital decompression. The medial orbital wall was identified in accordance with surgical procedures used in medial orbital decompression for thyroid eye disease (Figure 1E). The lamina papyracea was removed and the orbital periosteum was incised to allow orbital contents prolapsed (Figure 1F). The tumor was biopsied after periosteotomy. At the time of discharge, the patient’s visual acuity was 0.2 and the central limit flicker value was 20 Hz. Histology of the biopsy specimens of orbital lesions revealed atypical cells with eccentrically placed flattened nucleus and intracytoplasmic mucus positive for Periodic acid-Schiff (PAS) staining, which sporadically invaded muscle. These atypical cells were positive for cytokeratin (AE1/AE3) on immunohistochemistry. These findings were compatible with the metastasis of signet-ring cell carcinoma (Figure 2A-C). Postoperative CT showed that the orbital contents had prolapsed into the ethmoid sinuses (Figure 2D). Twelve months postoperatively, there was no recurrent orbital pain or visual deterioration although diplopia remained.
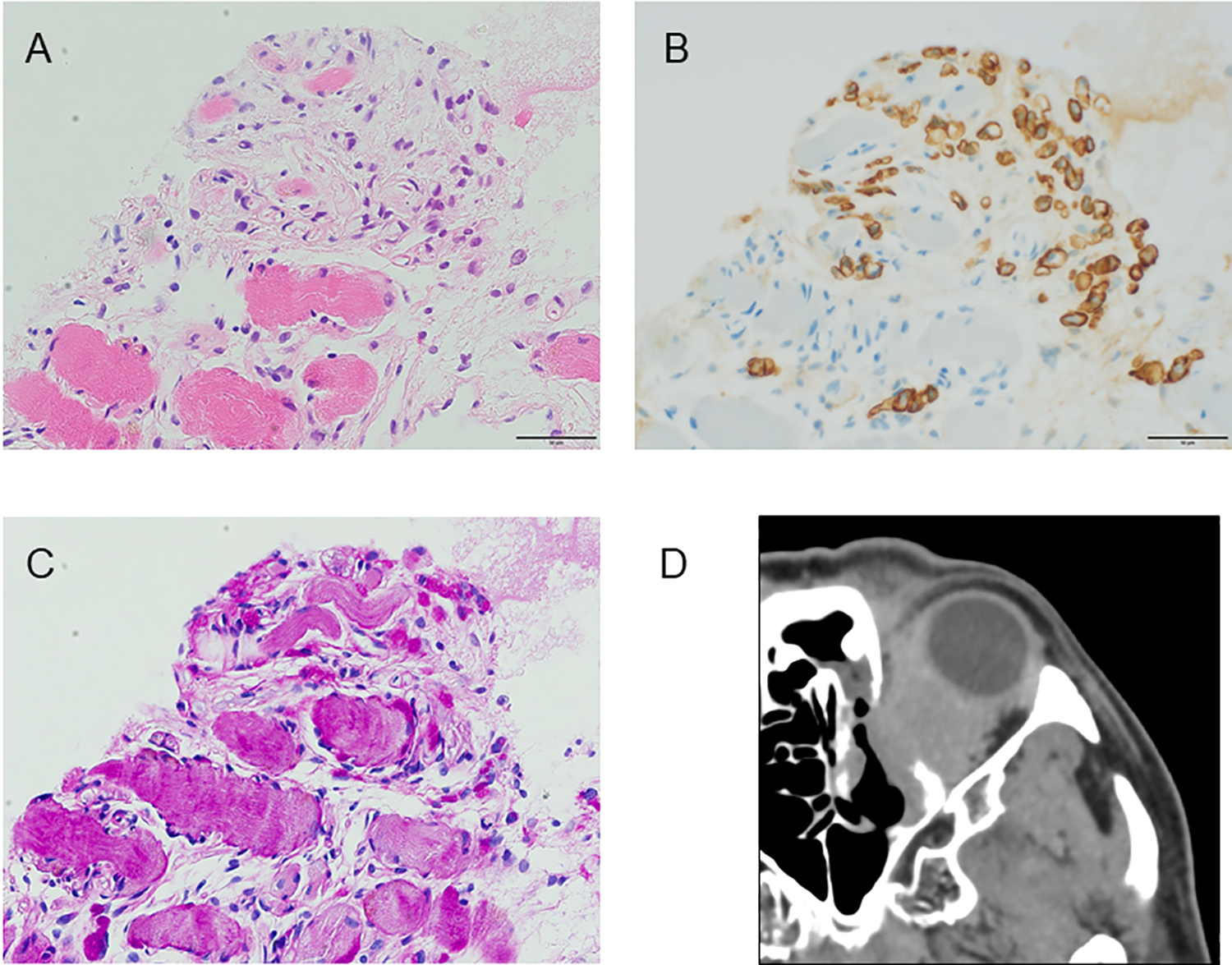
Histology of biopsy specimens of orbital lesions (scale bar size: 50 µm) and postoperative sinus CT, (A) Hematoxylin and Eosin (H&E) staining, (B) Immunohistochemical staining of cytokeratin (AE1/AE3), (C) Periodic Acid Schiff (PAS) staining, (D) Postoperative sinus CT: The orbital medial wall has been partially removed, and the intraorbital tumor is protruding into the nasal cavity.
Discussion
Signet ring cell carcinoma is a rare, high-grade adenocarcinoma. Primary SRCC tumors usually arise from the glandular cells of the stomach, but have also been reported in the breast, gallbladder, bladder, and pancreas.
Typical patterns of metastasis of SRCC of the stomach include peritoneal seeding, carcinomatous lymphangitis of the lung, and Krukenberg tumor. In contrast, intraorbital metastasis is very rare. Metastatic orbital tumors most commonly arise from breast cancer in women, lung cancer in men, and neuroblastoma in children. Metastatic orbital tumors are treated with radiation, chemotherapy, or chemoradiotherapy, but surgery may be an option for symptomatic relief. 2 Endonasal endoscopy is a viable approach in addition to the transconjunctival and skullbase routes. Endonasal endoscopic route has the advantage of providing a wide field of view and is minimally invasive. The medial and inferior portions of the orbit are suitable for the intranasal endoscopic approach because of their positions relative to the extraocular muscle and optic nerve. 3
In thyroid ophthalmopathy, medial orbital decompression is indicated in the active phase when steroid therapy and external radiation are ineffective, and in the inactive phase for the purpose of restoring visual function and improving cosmetic appearance. Restoration of visual acuity and decrease of ocular protrusion can be obtained by removing the medial wall of the orbit and incising the periosteum. 4
With regard to benign tumors, several studies reported that intranasal endoscopic orbital decompression or extraction from the inner side of the eye socket resulted in reduced ocular pain and improved ocular motility, visual field, and color vision. 3 In metastatic breast carcinoma, decompression was performed for palliative purposes. 5
In our case, partial removal of the orbital medial wall and periosteum was performed, and orbital pain and ocular protrusion were reduced by orbital decompression. In particular, the patient complained of orbital pain preoperatively, but it disappeared postoperatively. Because the tumor was located medial to the orbit, a definitive diagnosis could be made by performing a biopsy during the procedure. There is no consensus on palliative orbital decompression for intraorbital malignancies for symptomatic relief, but it may be a good option in some patients.
We report a very rare case of intraorbital metastasis of gastric SRCC. A biopsy by nasal endoscopy and medial orbital decompression were performed during a single procedure, which resulted in relief of orbital pain. In patients with intraorbital metastases of malignant tumors, orbital decompression surgery may be a useful option for palliative purposes.
Footnotes
Authors’ Note
Yukinori Tsuruta and Yohei Maeda contributed equally to this manuscript. Y.T., Y.M., Y.K., and M.H. performed surgery and reviewed the literature. Y.M. and S.N. made figures. T.T., K.T., A.N., S.O., E.M., and H.I. provided advice on the patient treatment and edited the manuscript. All authors participated in discussion of the results and approved the final draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.