
Abstract
Acute airway obstruction caused by invasive laryngeal cancer can make surgeons reluctant to perform a high-risk tracheostomy, which is life-saving for such patients. In the setting of the current COVID19 pandemic, we present a case of severe transglottic stenosis due to stage IV laryngeal carcinoma, in which gaseous exchange was facilitated by venovenous (VV) extracorporeal membrane oxygenation prior to emergent tracheostomy. The VV technique can ensure adequate oxygenation and CO2 removal. Venovenous extracorporeal membrane oxygenation provided sufficient time for surgical planning and preparation. It reduced the formation of aerosol, lowered the risk associated with life-saving tracheostomy, and protected the patient from ischemia.
Introduction
Emergent tracheostomy is an effective way to safeguard against impending airway obstruction caused by cancer of the larynx. However, for late-stage malignant lesions, such as those showing thyroid involvement, emergency tracheostomy is risky. In such cases, anatomic planes for tracheostomy are destroyed by tumor infiltration. In addition, the supine position may not be tolerated due to CO2 retention and respiratory muscle fatigue. These factors all increase the probability of significant hypoxia or severe hypoxemic cardiac arrest during tracheostomy. In the literature, some studies were found that used extracorporeal membrane oxygenation (ECMO) during high-risk interventional procedures, such as fiber-optic bronchoscopy, for airway stenosis caused by a malignant tumor. Inspired by these studies, and in the setting of the COVID-19 pandemic, we performed ECMO-assisted tracheostomy in a patient who presented with grade IV dyspnea and a diagnosis of stage IV transglottic carcinoma.
Case Report
A 66-year-old man presented to the emergency room with impending airway obstruction on March 13, 2020. He had complained of progressive hoarseness for almost 1 year. During the last 2 months, he experienced difficulty swallowing solid food, which resulted in loss of appetite and weight. However, he ignored this symptom and sought no medical help. One month prior, he experienced stridor. The travel history showed that neither the patient nor his relatives (wife and daughter) had contact with any confirmed or suspected case of COVID-19 within the previous 14 days. He had chronic atrial fibrillation (treated by catheter ablation) and a 40 pack-year smoking history. Physical examination revealed respiratory distress with stridor in a semi-recumbent position; the patient used the accessory muscles of respiration. A hard mass in the anterior triangle of the right side of the neck was palpated. Cervical lymph nodes were identified but were not hard and were mobile. A computed tomography (CT) scan of the neck (Figure 1) and laryngoscopy were conducted (Figure 2).
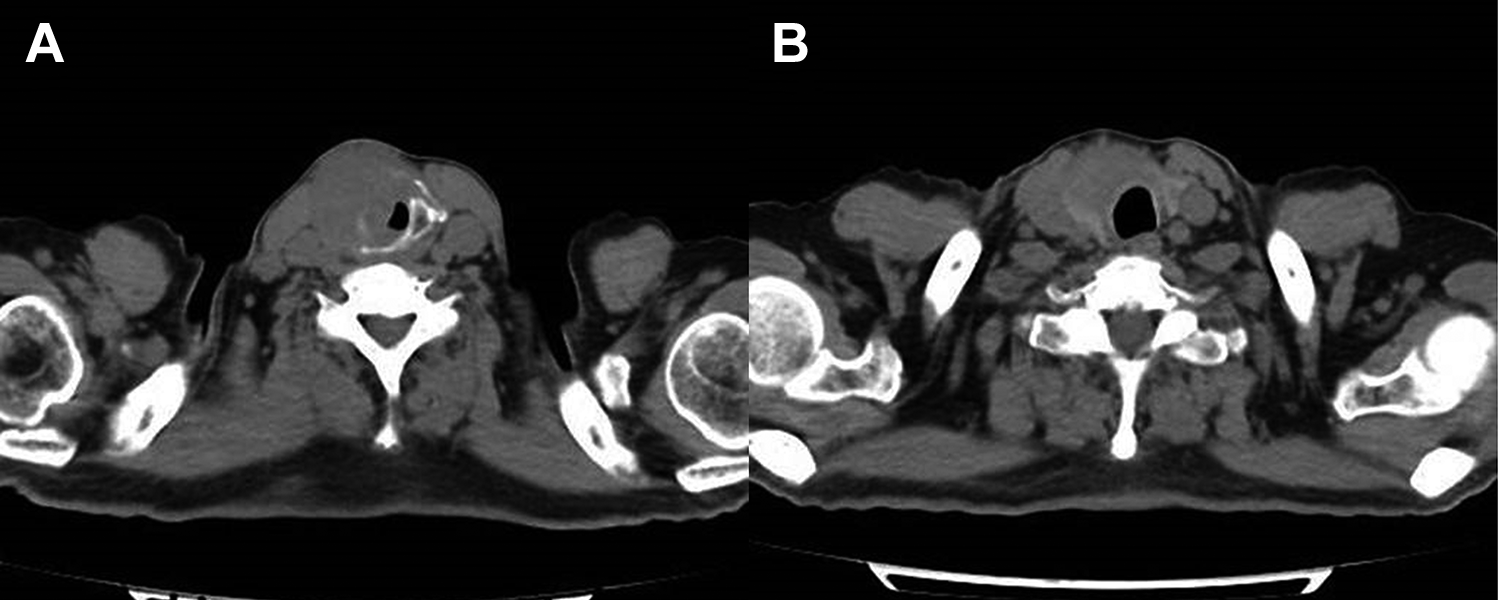
Computed tomography scan of neck showed that the tumor involved the right aryepiglottic fold, right vocal cord, right thyroid cartilage, and thyroid gland (A). The left vocal cord, and posterior and anterior commissures, suggested contralateral involvement; this was confirmed on pathology (B). There was no hypopharynx posterior wall involvement. The jugular chain lymph nodes were increased in number but not enlarged.
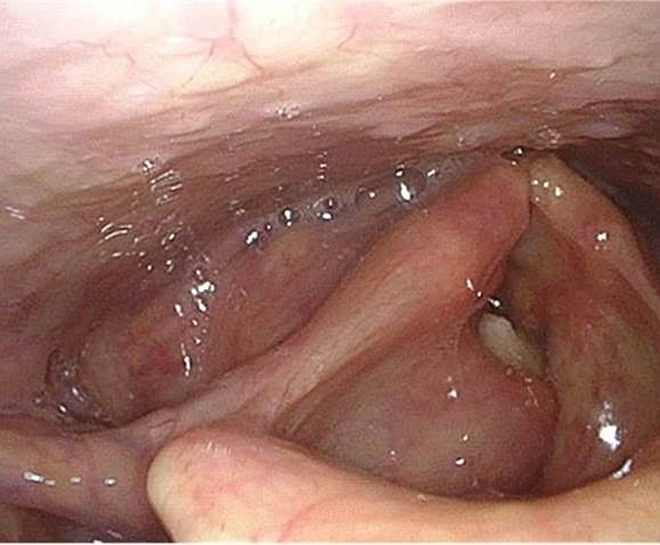
Flexible laryngoscopy performed in the clinic showed fixation of the right vocal cord and bulging of the ventricular band.
Although there were no new coronavirus cases in Beijing at that time except for imported cases, prevention and control was of great importance. Because the laryngeal lesion shared some symptoms with COVID-19, such as cough, sore throat, 1 and dyspnea, and given the existence of asymptomatic carriers, chest CT scan was considered and a molecular test of COVID-19 was conducted. A real-time reverse transcriptase polymerase chain reaction (RT-PCR) test for COVID-19 nucleic acid was performed using nasopharyngeal swabs (Novel Coronavirus PCR Fluorescence Diagnostic Kit; BioGerm Medical Biotechnology), which showed a negative result. COVID-19 antibodies were negative. Influenza A and B were also excluded. The C-reactive protein level and lymphocyte count were normal. He was oxygenating at 98% to 100% on 3 L O2 delivered by nasal cannula. A third-generation cephalosporin (ceftriaxone, 2 g) was combined with methylprednisolone (40 mg) and administered intravenously. However, the condition of the patient became much worse. A multidisciplinary team consisting of an otolaryngologist, anesthesiologists, and a respiratory intensive care unit (RICU) specialist discussed the patient. Anesthetic assessment ruled out front-of-neck airway access and intratracheal intubation because of the extent of the distortion of the anatomy by the transglottic carcinoma, and the inability of the patient to tolerate the supine position. The RICU specialist suggested placing the patient on venovenous (VV)-ECMO to ensure excellent oxygenation without the need for mechanical ventilation. This would provide more time to deal with the vascular tumor and help stabilize the surgical field. Therefore, VV-ECMO placement was conducted under local anesthesia with a right femoral-left jugular configuration. We then initiated VV extracorporeal life support at 3.5 L/min (3500 rpm, flow rate of 3 L/min) with arterial pressure monitoring. Intravenous anesthesia was induced and maintained with propofol and remifentanil. Before the start of the tracheostomy, all surgical staff wore personal protective equipment (PPE), including an N95 mask covered by another surgical mask, goggles and face shield, cap, double gloves, and a water-resistant disposable gown. 1,2 The patient was given mask oxygen in the supine position. A 4- to 5-cm horizontal incision at the level of the second ring of the trachea (1 cm below the cricoid) was made, so that the incision could be used in the future neck dissection and total laryngectomy. The incision was injected with 1% lidocaine with 1:100 000 epinephrine. After dividing the strap muscles, the thyroid isthmus was exposed together with the right lobe of the gland infiltrated by the tumor. We decided to cut though the thyroid isthmus but took great care to prevent bleeding from the edges. The pretracheal space was normal and no adhesions were found. The pretracheal fascia was cleared with blunt dissection and the tracheal rings were identified. A U-shaped Bjork flap was made, and an 8.5 tracheostomy tube was inserted through the opening. During the tracheostomy, the SaO2 ranged from 92% to 98%. After the patient woke up, his SaO2 was stable at over 96% without any extra oxygenation; thus, the VV-ECMO was removed in the operating room. The patient was taken to the intensive care unit for overnight monitoring followed by transfer to the ear, nose, and throat (ENT) ward the next day. A few days later, total laryngectomy was performed along with partial thyroidectomy. The pathology of the specimen was consistent with a transglottic squamous carcinoma with right thyroid lobe invasion. No metastatic carcinoma was seen in the lymph nodes (0 of 76). He was discharged home the following week.
Discussion
This case report demonstrates the successful use of VV-ECMO in the management of an extensive transglottic tumor causing impending acute airway obstruction and shows that ECMO can be used to maintain the oxygen level in cases of acute airway obstruction during awake tracheostomy. Maintaining the ventilation during a surgical procedure plays a vital role in relieving acute airway obstruction caused by laryngeal carcinoma. For stage IV transglottic carcinoma, tracheal stenosis is common and makes intubation impossible. The use of ECMO to manage ventilation during tracheostomy allows better visualization of the surgical site and obviates life-threatening hypoxia.
Extracorporeal membrane oxygenation is a life-support technique using mechanical devices to support both cardiac and respiratory function when the native systems fail. For this patient, whose cardiac function was normal, VV-ECMO was used to support the respiratory system. 3,4
Before tracheostomy, a CT scan showed that the tumor had grown into the right thyroid lobe. Considering that an invaded thyroid cannot easily be retracted upward with a double tracheal hook, we decided to cut through the isthmus. Although no adhesions were found, the thyroid tissue was more vascular than usual and it took much longer to stop the bleeding with bipolar coagulation. Mourad et al reported that only a small proportion of total resected thyroid specimens showed evidence of squamous cell carcinoma and concluded that surgical management of the thyroid gland should not be performed routinely except for subglottic and transglottic types. 5 Therefore, in this patient, following total laryngectomy, a partial thyroid lobectomy was conducted; the right thyroid was invaded by the tumor with a negative edge. When late-stage transglottic carcinoma prevents intubation and cricothyrotomy, ECMO may be used along with emergent tracheostomy to relieve airway obstruction.
Many surveys and publications have reported that the coronavirus can be transmitted by an asymptomatic carrier. 6,7 Our patient was assessed for COVID-19 according to his detailed travel history, a thoracic CT scan, and molecular testing. Compared with some other surgeons, ENT specialists are at high risk during clinical examinations and during invasive procedures performed in the respiratory tract or airway cavities (paranasal sinuses, middle ear). Thus, direct transmission of COVID-19 to ENT surgeons is of concern. Following the instructions provided by the government and World Health Organization, we wore PPE, including an N95 mask, cap, goggles, long-sleeved impervious gown, and gloves during the procedure. 8 For this patient, ECMO allowed intravenous anesthesia, which avoided the generation of aerosolized blood or tracheal secretions.
Conclusions
Venovenous-ECMO helped to improve ventilatory function during tracheostomy surgery performed in a patient with acute airway obstruction caused by transglottic squamous carcinoma. Usually, the cardiac function in such patients is stable, so the VV technique was sufficient to ensure adequate oxygenation and CO2 removal. In the setting of the COVID-19 pandemic, VV-ECMO provided sufficient time for surgical planning and preparation, which reduced the formation of aerosol, lowered the risk associated with life-saving tracheostomy, and protected the patient from ischemia. In this patient, the short-term prognosis after total laryngectomy following VV-ECMO-supported tracheostomy was acceptable.
Footnotes
Authors’ Note
Zhongyan Chen and Yong Lv contributed to the article equally. All procedures performed in studies involving human participants were in accordance with the ethical standards of the China-Japan Friendship Hospital Ethical Committee. Informed consent was obtained from individual participant involved in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.