
Abstract
A 27-year-old man was referred to our hospital for evaluation of a nasopharyngeal mass. He did not complain of any symptoms such as a runny nose, posterior nasal drip, nasal bleeding, or nasal congestion. There were no specific findings in his or his family’s history. Nasal endoscopy identified a small sized-papillomatous mass across the posterior nasal septum and nasopharyngeal vault (Figure 1A). No other specific findings were observed in the nasal cavity and sinuses. Computed tomographic (CT) scan of the nose and paranasal sinuses showed a 0.7-cm-sized lesion in the posterior septum of the nasopharynx. The lesion had a cotton swab appearance in the axial CT images, with the nasal septum being the stick part and the lesion being the cotton part (Figure 2A, B). The endoscopic approach was used to remove the mass. Normal mucosa was removed from the margin of the tumor by 2 ∼ 3 mm. After the removal of the tumor, electrocautery was performed on the tumor site. Histopathological examination of the mass found papillary proliferation at high magnification, and a core composed of fibrous tissue and vessels. All the cells surrounding the fibrovascular core were papillary adenocarcinoma cells (Figure 3). In immunohistochemistry, thyroid transcription factor (TTF)-1 and epithelial membrane antigen were positive, and thyroglobulin and S-100 protein were negative. Based on these, the specimen was confirmed as nasopharyngeal papillary adenocarcinoma. No metastases were found in the postoperative PET (positron emission tomography)-CT examination, and there were no specific findings during thyroid ultrasonography. There was no relapse for a year and a half after the surgery.
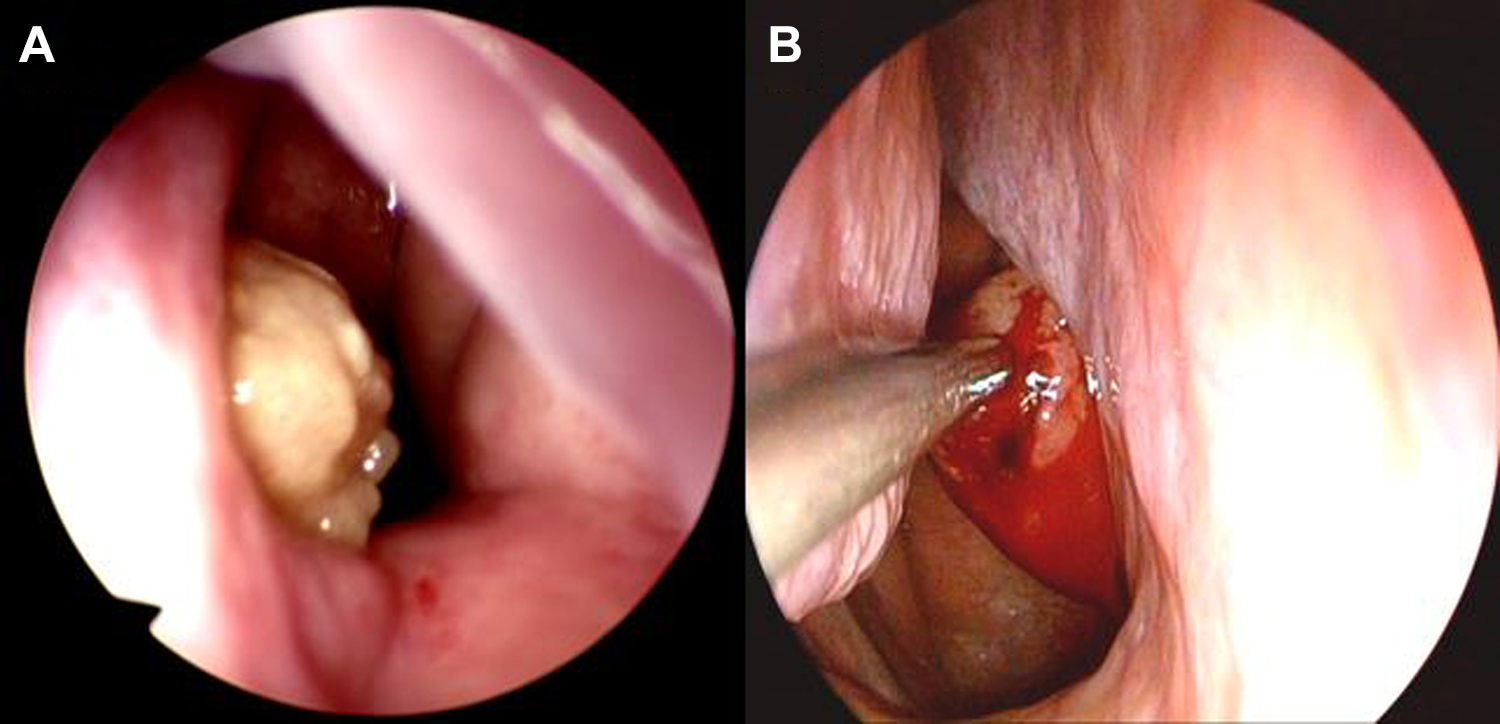
A and B, Nasal endoscopy showing a papillomatous mass attached to the posterior nasal septum and the vault of the nasopharynx in the first and second cases, respectively.
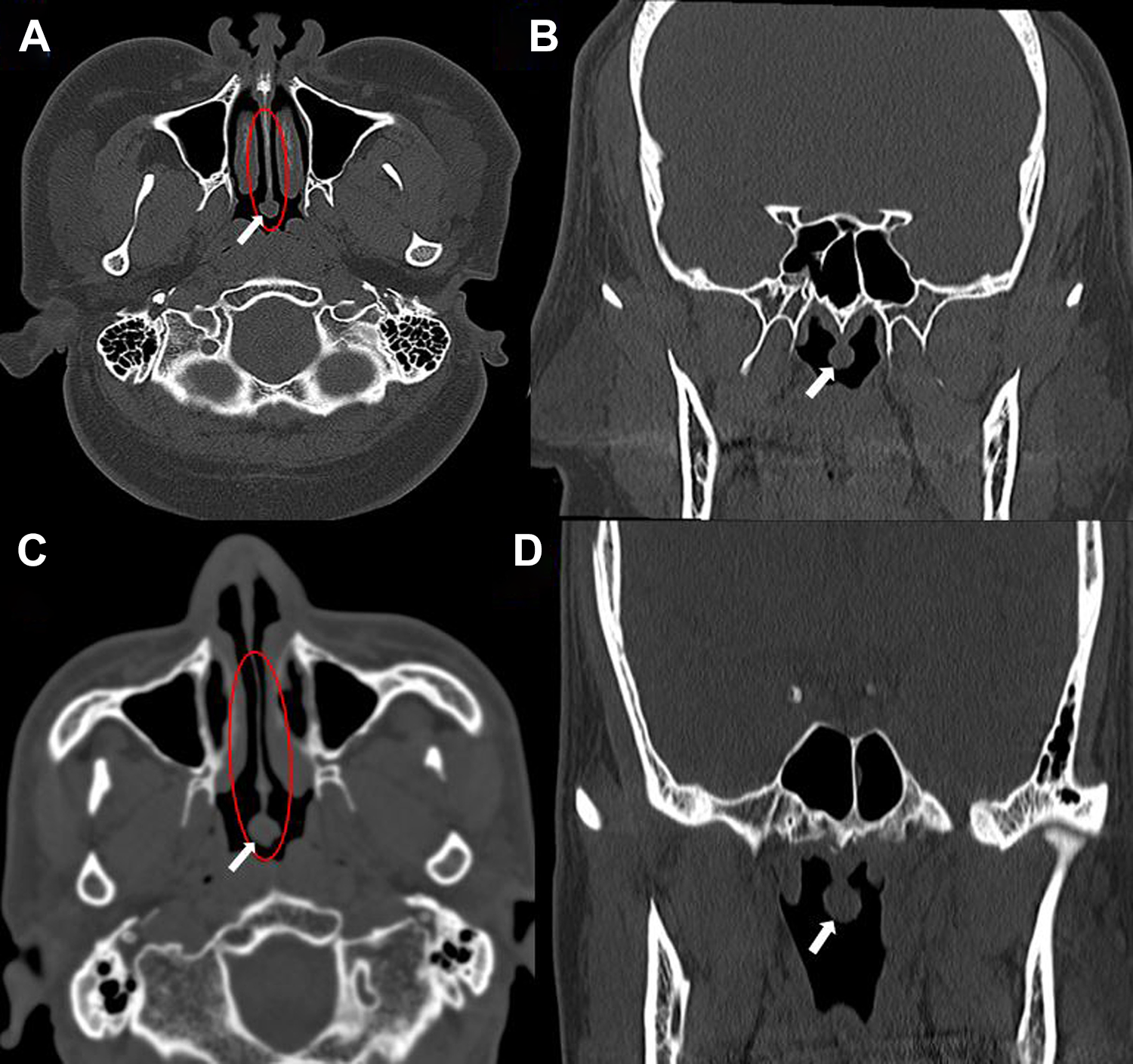
A and B, Axial and coronal computed tomographic (CT) scans showing a 0.7 cm-sized lesion (arrow) in the posterior septum of the nasopharynx in the first case. C and D, Axial and coronal CT scans showing a 1 cm-sized lesion (arrow) in the posterior septum of the nasopharynx in the second case. The red circles indicate the cotton swab appearance of the lesions in the axial CT scans, with the nasal septum being the stick part and the lesion being the cotton part.
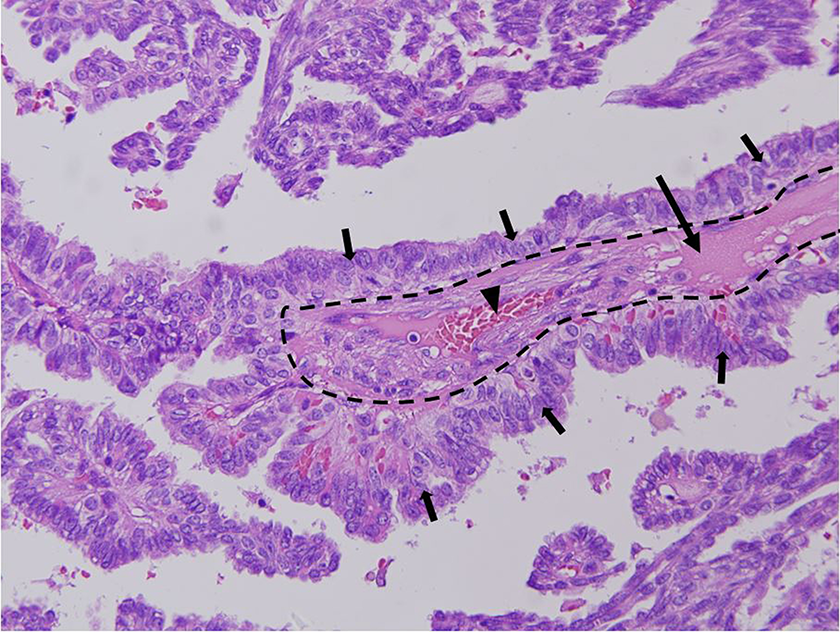
Histopathological findings of the mass showing papillary proliferation at high magnification, with the core (dotted line) composed of fibrous tissue (long arrow) and vessels (arrowhead). All cells surrounding the fibrovascular core are papillary adenocarcinoma cells (short arrows). (H&E staining, ×400).
A 51-year-old man visited our hospital to address a posterior nasal drip with intermittent bleeding that had occurred a month before. The patient did not complain of any other symptoms such as a runny nose or nasal congestion. There were no specific findings in his or his family’s history. Nasal endoscopy demonstrated a 1-cm-sized papillomatous mass across the posterior nasal septum and the nasopharyngeal vault. The mass was easily hemorrhagic when touched (Figure 1B). No other specific findings were observed in the nasal cavity or sinuses. Computed tomographic scans of the nose and paranasal sinuses showed a 1-cm-sized lesion in the posterior septum of the nasopharynx. The lesion had a cotton swab appearance in the axial CT images, with the nasal septum being the stick part and the lesion being the cotton part (Figure 2 C, D). Surgery was performed in the same manner as in the first case. Histopathological examination identified the mass as nasopharyngeal papillary adenocarcinoma. No metastases were found in the postoperative PET-CT examination, and there were no specific findings during thyroid ultrasonography. There was no relapse for 3 years after surgery.
Nasopharyngeal cancers are divided into nasopharyngeal carcinoma, nasopharyngeal papillary adenocarcinoma, and salivary gland tumors. The most common type is nasopharyngeal carcinoma. Adenocarcinoma in the nasopharynx is a very rare disease. 1 The histopathology of nasopharyngeal papillary adenocarcinoma is very similar to that of thyroid papillary carcinoma. In immunohistochemical staining, both carcinomas are positive for TTF-1, so differentiation between them is essential. Thyroid papillary carcinoma is also positive for thyroglobulin, while nasopharyngeal papillary adenocarcinoma is not. 2 In nasopharyngeal papillary adenocarcinoma, perineal and vascular lymphatic invasion are not observed, and metastasis was not reported, so the prognosis is very good. 3 We report here on 2 cases of nasopharyngeal papillary adenocarcinomas. The lesions were relatively small in size and showed a cotton swab appearance in axial CT images. Thus, if a nasopharyngeal mass shows a cotton swab appearance in axial CT images, it can be suspected for nasopharyngeal papillary adenocarcinoma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.