
Abstract
Objective:
To study anterior nasal spine fractures, including the incidence, missed diagnosis rates, and relationship with shapes using computed tomography (CT).
Methods:
Two hundred cases of axial CT images performed for maxillofacial trauma were reviewed. The incidence, correct, and missed diagnosis rates of anterior nasal spine fractures were studied. The relationship between the fracture and the shape of the anterior nasal spine was also analyzed.
Results:
The rate of anterior nasal spine fractures was 22.00% (44 of 200). The diagnostic accuracy was 4.55% (2 of 44) and the missed diagnosis rate was 95.45% (42 of 44). The fracture rates of the double rod, single rod, triangle, and irregular anterior nasal spine were 33.85% (22 of 65), 32.26% (10 of 31), 12.24% (12 of 98), and 0.00% (0 of 6), respectively. The double and single rod types of anterior nasal spine were most likely to be fractured than the type of triangle (χ2 = 11.05, 6.67, P < .0167). No fracture was found in the irregular type of anterior nasal spine.
Conclusion:
Anterior nasal spine fractures are not rare and the high missed diagnostic rate results from unfamiliarity with the structure. Double and single rod types of anterior nasal spines are easy to fracture. Bony reconstruction and thin thickness of CT images are necessary for diagnosis.
Introduction
The anterior nasal spine is the part of the maxilla that protrudes forward in the middle of the lower edge of the piriform aperture. The anterior nasal spine is a thin bony structure that is easily fractured. The literature pertaining to the anterior nasal spine and its fractures is limited.1-4 Fracture of the anterior nasal spine is considered to be rare based on the extant literature. Because the anterior nasal spine is usually ignored by physicians, 1 anterior nasal spine fractures are often missed. In the present study, the incidence and rate of missed diagnosis of anterior nasal spine fractures were analyzed, as was the relationship between the shape of the structure and such fractures. The main purpose of our study was to make clinical physicians, including radiologists, aware of the existence of the anterior nasal spine, and its fractures.
Materials and Methods
Patients
Two hundred patients with maxillofacial trauma who underwent a maxillofacial computed tomography (CT) examination between January 2016 and January 2017 in our hospital were enrolled in the study, including 129 males and 71 females (age range, 3-89 years; average age, 37 ± 17 years). This study was approved by the hospital’s ethics committee and consent was obtained from all patients.
Examination
Computed tomography scans were performed using a 128-slice CT scanner (Discovery CT 750HD; GE Healthcare), 16-slice CT scanner (Light Speed; GE Healthcare), and a 64-slice CT scanner (Siemens Cardiac Sensation 64; Siemens Medical System). The CT protocols were as follows: spiral scan mode; pitch = 1; layer thickness, 1 mm; and interval, 0.6 mm. The bone algorithm (kernel = 60) reconstruction was used to observe the bone with a CT window width of 2000 Hu and window level of 300 HU. The soft tissue algorithm (kernel = 35) was used to observe the soft tissue surrounding the bone with a CT window width of 300 HU and a window level of 60 HU.
Analytic Method
Transverse CT images of 200 patients with maxillofacial trauma were reviewed by 2 musculoskeletal radiologists who had >10 years of experience. The incidence of anterior nasal spine fractures, and the correct and missed diagnosis rates of original reports for the anterior nasal spine fractures were counted based on the axial CT images. The rates of different types of anterior nasal spine fractures were calculated. The relationship between the fracture and the shapes of the anterior nasal spine was analyzed. The 2 radiologists consulted with each other to achieve agreement if different opinions existed.
The anterior nasal spine was divided into 4 types according to the morphology on axial CT, as follows: double rod type (Figure 1); single rod type (Figure 2); triangular (Figure 3); and irregular type (Figure 4).The axial section displaying the maximal range of the anterior nasal spine was selected to define the type. The shape with 2 upright thin stripe structures disjointed from each other was defined as the double rod type, the shape of the single thin stripe structure was defined as the single rod type, the anterior nasal spine with a triangular shape was defined as the triangular type, and the other shapes were classified as the irregular type.
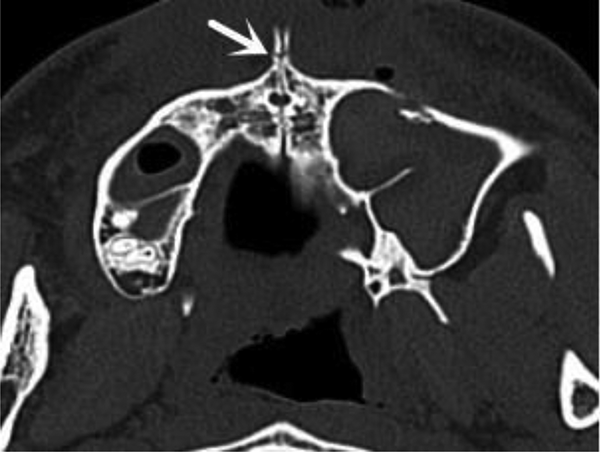
Axial CT image of a 24-year-old man with a double rod-type anterior nasal spine fracture (arrow). CT indicates computed tomography.
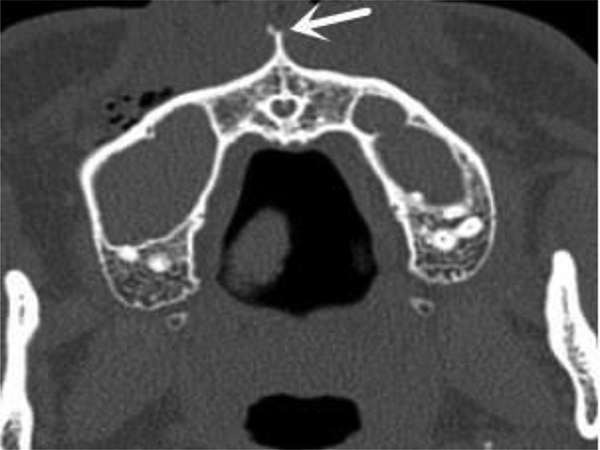
Axial CT image of a 16-year-old girl with a single rod-type anterior nasal spine fracture (arrow). CT indicates computed tomography.
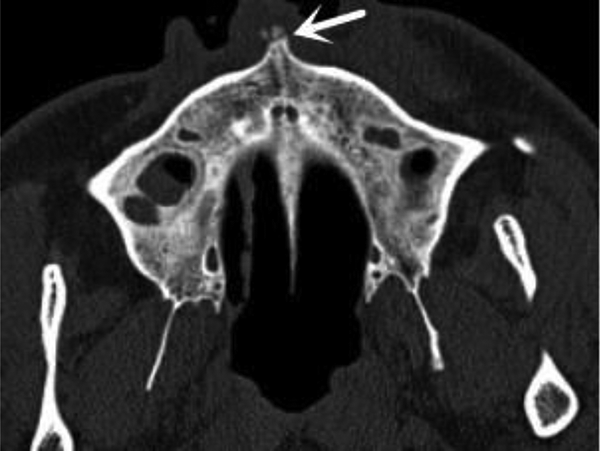
Axial CT image of a 33-year-old man with a triangular-type anterior nasal spine fracture (arrow). CT indicates computed tomography.
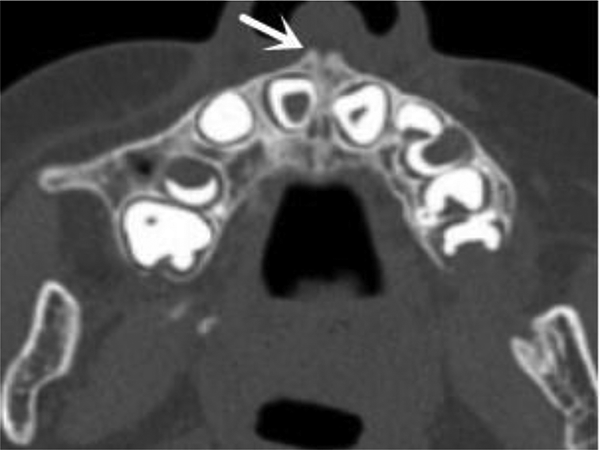
Axial CT image of 12-year-old boy with an irregular-type anterior nasal spine without fracture (arrow). CT indicates computed tomography.
Statistical Method
The 4-fold table method was utilized to calculate χ2 values and the test level was corrected using the Bonferroni method. The α value was 0.05/3 = 0.0167. A pairwise comparison was used for multiple sets of data in the same group.
Results
Incidence of Anterior Nasal Spine Fractures
Forty-four cases of anterior nasal spine fractures were detected based on CT in 200 patients with maxillofacial trauma; the incidence of anterior nasal spine fractures was 22.00% (44 of 200).
Type of Trauma Causing Anterior Nasal Spine Fractures
Forty-four cases of anterior nasal spine fractures were caused by a variety of trauma, including 19 car accidents, 10 boxing injuries, 12 fall injuries, and 3 cases of unknown trauma.
Effect of Reconstruction Algorithm on Displaying Anterior Nasal Spine Fractures
The CT axial images with a soft tissue algorithm showed 19 anterior nasal spine fractures (19 [18%] of 44 43) and 25 suspected fractures (25 [56.82%] of 44). All 44 cases (44 [100%] of 44) of anterior nasal spine fractures were correctly diagnosed on axial CT images with bone algorithm showing distinct fracture lines.
Correct and Missed Diagnosis Rates of Original Reports for Anterior Nasal Spine Fractures
Only 2 cases of the fracture were diagnosed in the original CT reports. The correct diagnosis rate was 4.55% (2 of 44) and the missed diagnosis rate was 95.45% (42 of 44).
Relationship Between Fractures and the Shape of the Anterior Nasal Spine
The fracture rates of different types of anterior nasal spines were as follows: double rod (33.85% [22 of 65]; Figure 1); single rod (32.26% [10 of 31]; Figure 2); triangular type (12.24% [12 of 98]; Figure 3); and irregular type (0.00% [0 of 6]; Figure.4). The double and single rod types of anterior nasal spines were more prone to fracture than the triangle type (χ2 = 11.05, 6.67, P < .0167). There was no significant difference in fracture rates between the double and single rod types of anterior nasal spines (χ2 = 0.02, P > .05).
Relationship Between Fractures of the Anterior Nasal Spine and Nasal Bone
Of the anterior nasal spine fractures, 93.18% (41 of 44) were accompanied by nasal bone fractures. Of nasal bone fractures, 39.42% (41 of 104) were accompanied by anterior nasal spine fractures.
Discussion
Anatomy and Morphology of the Anterior Nasal Spine
The anterior nasal spine is a tiny bony tubercle located at the edge of the maxilla piriform aperture. It has been shown that the anterior nasal spine exhibits the following characteristics 5 slight, intermediate, and marked. The slight characteristic indicates minimal to no projection beyond the inferior nasal aperture. The intermediate characteristic indicates a moderate projection of the anterior nasal spine beyond the inferior nasal aperture. The marked characteristic indicates a pronounced projection of the spine beyond the inferior nasal aperture. This classification, however, does not reflect the relationship between the morphologic characteristics of the anterior nasal spine and vulnerability of the anterior nasal spine. In our former studies, we observed the anterior nasal spine in 1000 maxillofacial patients using transverse CT and divided the anterior nasal spine into 4 types based on morphology, as follows: double rod (Figure 1); single rod (Figure 2); triangular (Figure 3); and irregular (Figure 4).
Clinical Value of Studying Anterior Nasal Spines and Fractures
The anterior nasal spine is a major anatomic landmark for surgery involving the maxillofacial region and dental procedures. The anterior nasal spine also plays an important role in clinical nasal endoscopic sinus surgery. For example, the anterior nasal spine is a reliable landmark to determine the occlusal vertical dimension in patients who have lost this vertical component. 6 The vector from the anterior nasal spine to the rhinion is very useful for measuring nasal root deviation. 7 The anterior nasal spine is often chosen as the measurement basis for positioning of the olfactory foramina and is important in determining the morphology of the human face with respect to support for the nasal tip and projection of the nose and upper lip. 8 In addition, when dissecting the sphenopalatine artery territory, it is beneficial to measure the depth and angle between the anterior nasal spine and the anterior and posterior margins of the sphenopalatine foramen, as well as the approximate diameter of the sphenopalatine foramen, which will help reduce the risk of injury and promote precise positioning in sphenopalatine artery surgery.
Even though the anterior nasal spine has been suggested as an important landmark for location9-11 and the anterior nasal spine is easily fractured, the nasal spine has not been the focus of relevant studies. Even though fractures in this area do not require surgery when nondisplaced in most cases, the diagnosis of anterior nasal spine fractures is significant and important in forensic science for sentencing.
Modalities to Detect Anterior Nasal Spine Fractures and the Advantages of CT
The anterior nasal spine is a very small structure, thus demonstrating fractures on radiographs is difficult. The cortex of this small structure has a low intensity on MRI, which also makes fractures difficult to detect. The anterior nasal spine is a bony structure with a high attenuation, however, and the long axis is in the front-to-back direction so that the anterior nasal spine is easy to display on CT axial images. Multislice helical CT scans form axial and isotropic reconstructed images in any plane (including coronal and sagittal planes) with a minimum thickness of 0.5 mm. Three-dimensional stereoscopic images can also be obtained by CT. Those types of CT images are helpful for observing the anterior nasal spine. In spite of this, the axial image of CT scans is the most basic and easily accessible.
The image algorithm has an important effect on the display of anterior nasal spine fine structure. The bone algorithm (a high-resolution algorithm) and thin thickness increase the spatial resolution but decrease the density resolution of CT images. Although the density resolution can be improved by using the soft tissue algorithm, the spatial resolution is reduced. The nasal spine is a bony structure with high density or attenuation, and the bone algorithm can significantly improve the spatial resolution and sharpness of the edge of the fracture line, thereby increasing the detection of fractures. The reduction in density resolution caused by the bone algorithm is not sufficient to have a visually significant effect on the nasal spine structure because the high-density bony structure exhibits a strong contrast with the surrounding soft tissue. The reduction in the spatial resolution of the soft tissue algorithm, however, will cause the edge of the fracture line to be blurred and thus affect detection of fractures. Therefore, the bone algorithm with high spatial resolution is better than the soft tissue algorithm in demonstrating fractures, including the anterior nasal spine. In the current study, 25 cases of suspicious fractures on the soft tissue algorithm images were retrospectively diagnosed to be fractures on the bone algorithm images. Therefore, both the thin layer and bone algorithm are necessary for detection of anterior nasal spine fractures.
Incidence, Correct, and Missed Diagnosis Rates of Anterior Nasal Spine Fractures
An anterior nasal spine is so small that it is easy to be overlooked, and many physicians, including radiologists, are unaware of its existence and turn a blind eye to this structure, giving rise to a high fracture misdiagnosis rate. Based on the extant literature, fractures of the anterior nasal spine are rare, 1 and only 4 cases have been reported (1 case diagnosed by CT and 3 cases by plain film radiographs).1-4 In the present study, however, 44 anterior nasal spine fractures were identified based on CT examinations in 200 patients with maxillofacial trauma. Although nearly one-fourth of patients had nasal spine fractures (22.00% [44 of 200]), only 2 patients were originally diagnosed by CT. The correct diagnosis rate was only 4.55% (2 of 44), while the missed diagnosis rate was as high as 95.45% (42 of 44). Initially, we were unaware of this bony structure and missed a case of a fracture of an “unknown structure” located in the maxillary midline area. When the case was questioned by a forensic physician, we reviewed the CT images and noticed this structure and the fracture. After consulting anatomic textbooks, we added the diagnosis of an anterior nasal spine fracture. Most et al 4 concluded that anterior nasal spine fractures are rarely reported, but we found that fractures involving this structure might not be as rare as described in the literature. Indeed, it was a lack of awareness of the anterior nasal spine that resulted in missed diagnosis of fractures. Once the existence of this structure was realized, there was no difficulty in diagnosing fracture of the anterior nasal spine on CT images.
Relationship Between Fractures and the Shape of the Anterior Nasal Spine
Whether or not the anterior nasal spine sustains a fracture is associated with the morphologic type. There have been no reports with respect to the relationship between the morphology of the anterior nasal spine and fractures. In the present study, the fracture rates of double rod, single rod, and triangular anterior nasal spines were 33.85% (22/65), 32.26% (10/31), and 12.24% (12/98), respectively. Double and single rod-type anterior nasal spines are easily fractured because of the long, thin slender bone structure that is unstable, while the triangular type is more stable and the probability of fracture is relatively low.
Type of Trauma Causing Fractures of the Anterior Nasal Spine
Either direct or indirect injuries involving the anterior nasal spine can give rise to fractures, which is related to the fragile anatomic structure. It has been reported in the literature that nasal bone fractures account for 59.3% of maxillofacial fractures caused by trauma. In the present study, 44 anterior nasal spine fractures were caused by a variety of trauma types, including car accidents, boxing injuries, falls, and unknown trauma types.
Relationship Between Anterior Nasal Spine Fractures and the Nasal Bone
In the current study, anterior nasal spine fractures often coexisted with nasal bone fractures because the anterior nasal spine is located in an area adjacent to the nasal region and trauma to the facial nasal region can easily affect the anterior nasal spine. In the present study, 93.18% of anterior nasal spine fractures were accompanied by nasal bone fractures, and of nasal bone fractures, 39.42% were accompanied by anterior nasal spine fractures. Therefore, when nasal bone fractures are demonstrated, special attention should be paid to the morphology of the anterior nasal spine to reduce missed diagnoses of fractures. While not all radiologists will routinely comment on anterior nasal spine fractures in association with fractures of nasal bones and maxilla, even when present, we suggest that this finding be identified by surgeons and noted on imaging due to the importance of the structure as a landmark and for structural support.
How to Avoid Missed Diagnoses
The anterior nasal spine is a small bony protrusion above the alveolar bone, located in the midline of the maxilla and at the bottom of the nose and the lower edge of the piriform aperture. Familiarity with the location of anterior nasal spine and attention given to the anterior nasal spine would help to avoid missed diagnoses (Figure 5).
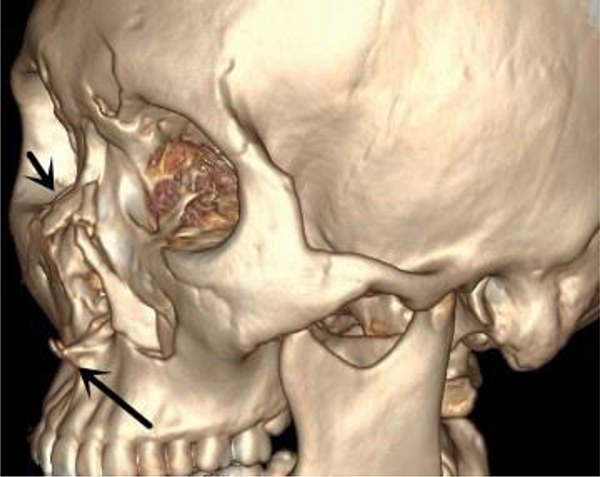
Volume rendering (VR) image of the patient in Figure 1 with nasal bone (short arrow) and anterior nasal spine fractures (long arrow).
Conclusion
Fractures of the anterior nasal spine in maxillofacial trauma are not uncommon (22.00%). The missed diagnosis rate of anterior nasal spine fractures is very high (95.45%) because this structure is overlooked. Double and single rod types of the anterior nasal spine are easily fractured. Bony reconstruction and thin thickness are necessary for confident diagnoses of anterior nasal spine fractures.
Footnotes
Acknowledgment
The authors thanks for Yanjie Meng’s great contribution to the article. Yanjie Meng makes equal contributions as much as the first author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.