
Abstract
Middle ear myoclonus (MEM) is a rare idiopathic clicking-type tinnitus attributed to abnormal contractions of the stapedius and/or tensor tympani muscles. 1 Most cases of MEM can be managed with medication, behavioral therapy, and avoidance of trigger factors. 2 In patients with intractable MEM, middle ear tendon resection (METR) is a treatment of choice with a high success rate. 3 However, reattachment of the resected tendon can occur in the healing process. 3 Herein, we present the first report of an MEM concomitant with eye blinking treated by resection of the tensor tympani tendon and the cartilage block insertion, which can prevent a recurrence.
A 73-year-old male presented with the complaint of clicking-type tinnitus concomitant with eye blinking for 2 years. Audiometry showed bilateral moderate sensorineural hearing loss. Nasopharyngoscopy demonstrated patent Eustachian tubes and no palatal myoclonus. Otoscopy showed the to-and-fro movement of the bilateral tympanic membrane with eye blinking. The tympanogram and acoustic reflex decay revealed irregular perturbations synchronous with eye blinking, which were normal without eye blinking (Figure 1). The brain magnetic resonance imaging revealed no evidence of cerebellar or brain stem causes. The patient was reassured and prescribed anticonvulsants and muscle relaxants after the diagnosis of MEM. However, the patient showed no response and requested surgical management. An endoscopic middle ear exploration was performed under local anesthesia via a transcanal approach. After elevating the tympanomeatal flap, we removed the posterior bony rim scutum to obtain a proper view of the stapedial tendon. We identified the retraction of the only tensor tympani tendon with eye blinking. The tensor tympani tendon was resected with the crurotomy scissor, and the tinnitus was completely resolved immediately. A thin-sliced small tragal cartilage block (1 mm × 1 mm) was inserted between cutting planes of the tensor tympani tendon to prevent reattachment (Figure 2; Supplemental Video). The tympanomeatal flap was returned to the native position. The patient has been under observation for 6 months without recurrence, hyperacusis, hearing loss, or other complications.
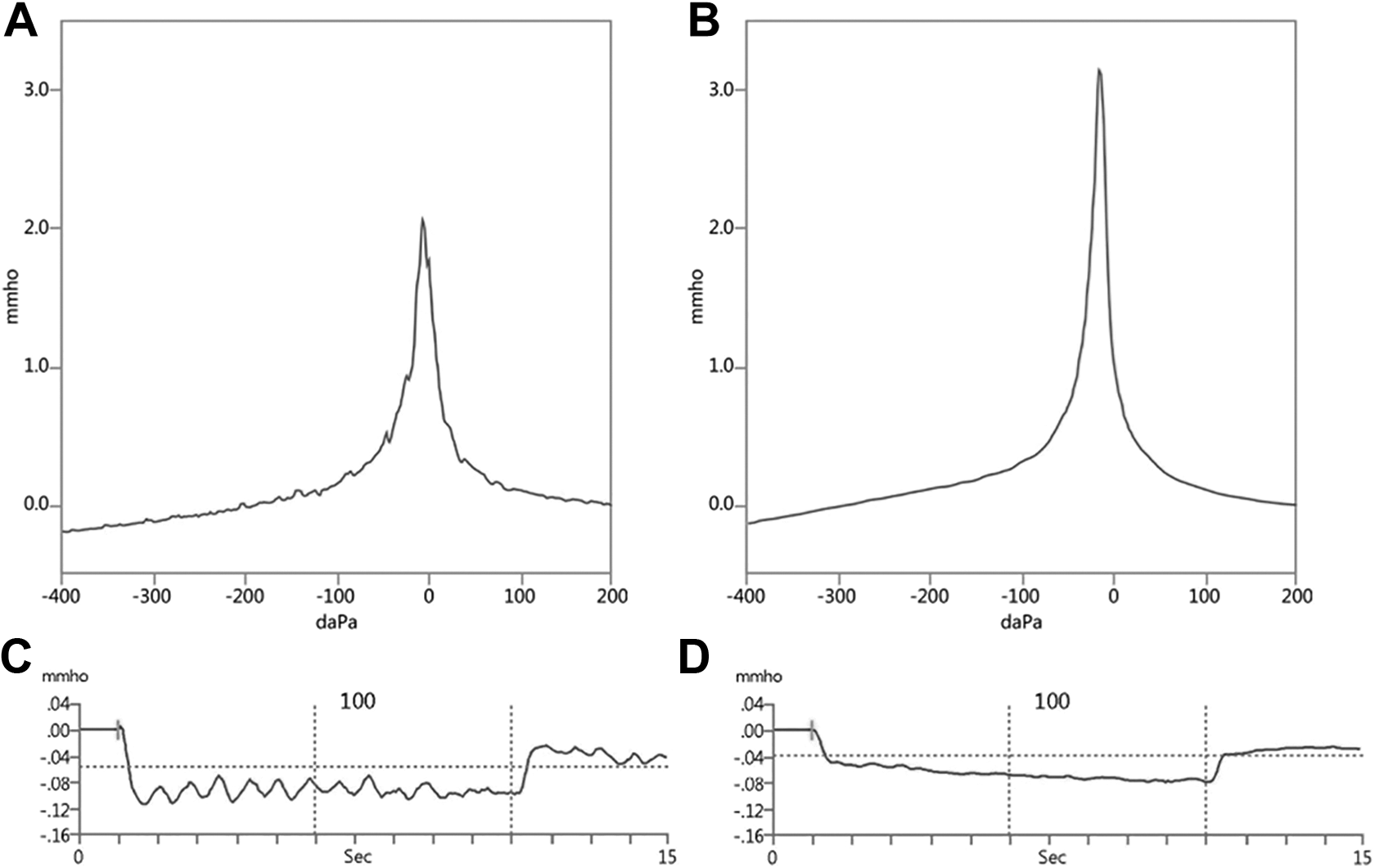
Tympanogram and acoustic reflex decay test. Tympanogram and acoustic reflex decay show irregular perturbations synchronous with eye blinking (A and C), which is normal without eye blinking (B and D).
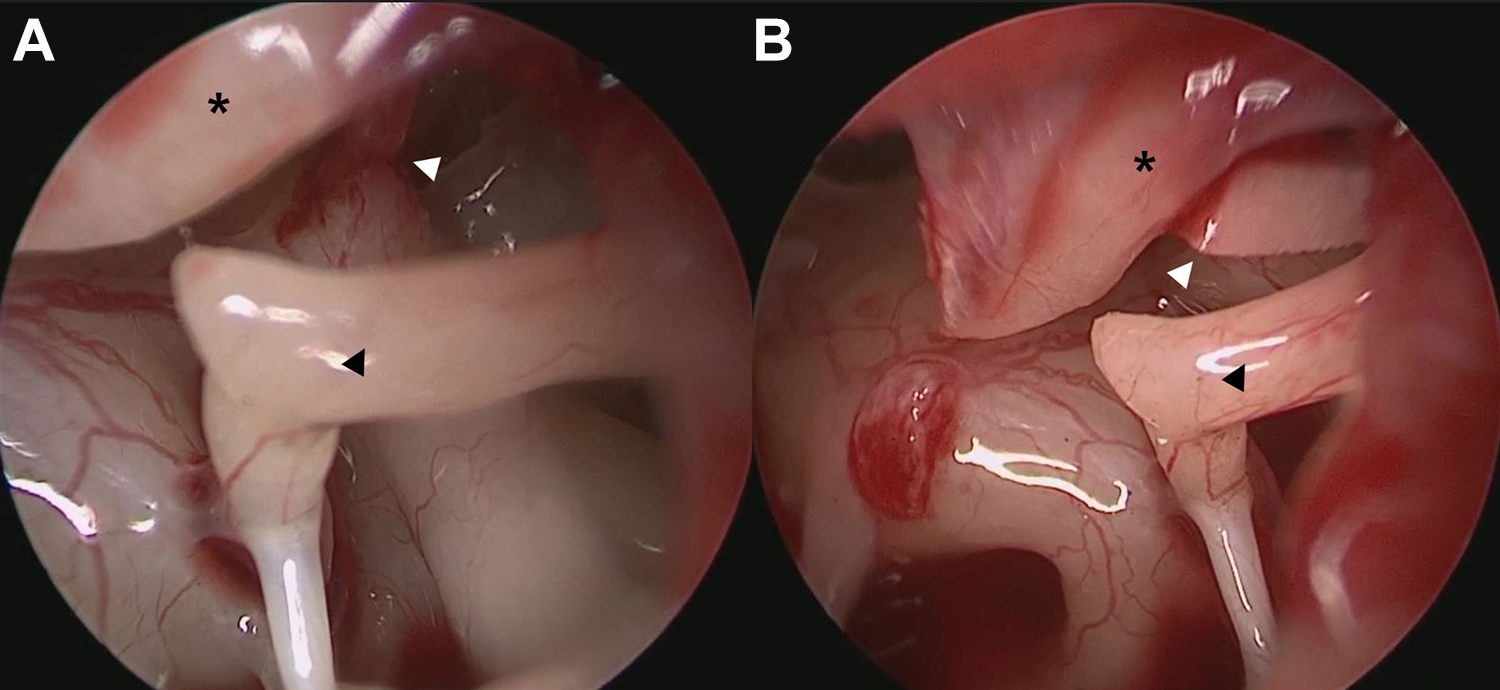
Intraoperative view of a middle ear. A, Resected tensor tympani tendon and cutting planes (white arrowhead). B, The tragal cartilage block (white arrowhead) was inserted between cutting planes of the tensor tympani tendon. Black asterisk, malleus; black arrowhead, incus.
Tinnitus due to the MEM is uncommon, and its etiology remains unclear. Loud noise, anxiety, and brainstem or cerebellar lesions have been suggested as possible causes, though most of the cases are idiopathic. 4 The perturbations on the acoustic reflex decay test and inspection of the tympanic membrane using an endoscope or microscope are the most reliable diagnostic tools.1,3 In the case of newly developed MEM, the brain magnetic resonance imaging should be performed because the lesion of brainstem or cerebellum may be the cause.2,4 For treatment, medications (muscle relaxant, anxiolytics, and anticonvulsants) are often used as the first therapeutic option. 2 If conservative therapy fails, METR could be considered.1-3 Park et al reported that 92% of the patients showed complete resolution after METR in their large case series. 3 To prevent recurrence due to incomplete resection or reattachment of the resected margin, they adopted a weak cauterization of the section site using the specially designed tip. 3 However, there is a possible risk of thermal injury to the facial nerve with electrocauterization; therefore, a laser may be an alternative. 3 Nevertheless, the problem is that not all clinics have specially designed tips or laser systems.
Hence, we placed a tragal cartilage block between cutting planes of the tensor tympani tendon. The cartilage block works as an obstacle that prevents the resected margins from being reconnected with a fibrous band and acquiring tension. Also, since the manipulation of the cartilage block is not difficult, the possibility of damage to surrounding structures is also low. Although additional tragal cartilage harvesting is required, it is worth conducting because it is a simple and safe technique that can be performed in a short time. 5
In conclusion, if making a sufficient gap between resected tendon is difficult due to an inaccessible anatomical structure or lack of appropriate surgical instruments in METR, cartilage insertion between the cutting planes of the tensor tympani tendon could be an alternative procedure to avoid MEM recurrence.
Supplemental Material
Supplemental Material, Patient_consent_form_1 - Tinnitus Concomitant With Eye Closure Treated by Tensor Tympani Tendon Resection and Cartilage Block Insertion
Supplemental Material, Patient_consent_form_1 for Tinnitus Concomitant With Eye Closure Treated by Tensor Tympani Tendon Resection and Cartilage Block Insertion by Seokhwan Lee, Soo-Keun Kong, Se-Joon Oh and Sung-Won Choi in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by clinical research grant from Pusan National University Hospital in 2020.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.