
Abstract

A 76-year-old woman presented with a several year history of a sensation of a lump in the throat, hoarseness, and frequent throat clearing. She had been diagnosed with gastroesophageal reflux disease (GERD) 8 years earlier. She denied smoking and alcohol consumption. Laryngoscopy showed multiple cobblestone-like pachydermia changes (Figure 1) on the mucosa of the interarytenoid and postcricoid regions, suggesting a diagnosis of laryngopharyngeal reflux (LPR).
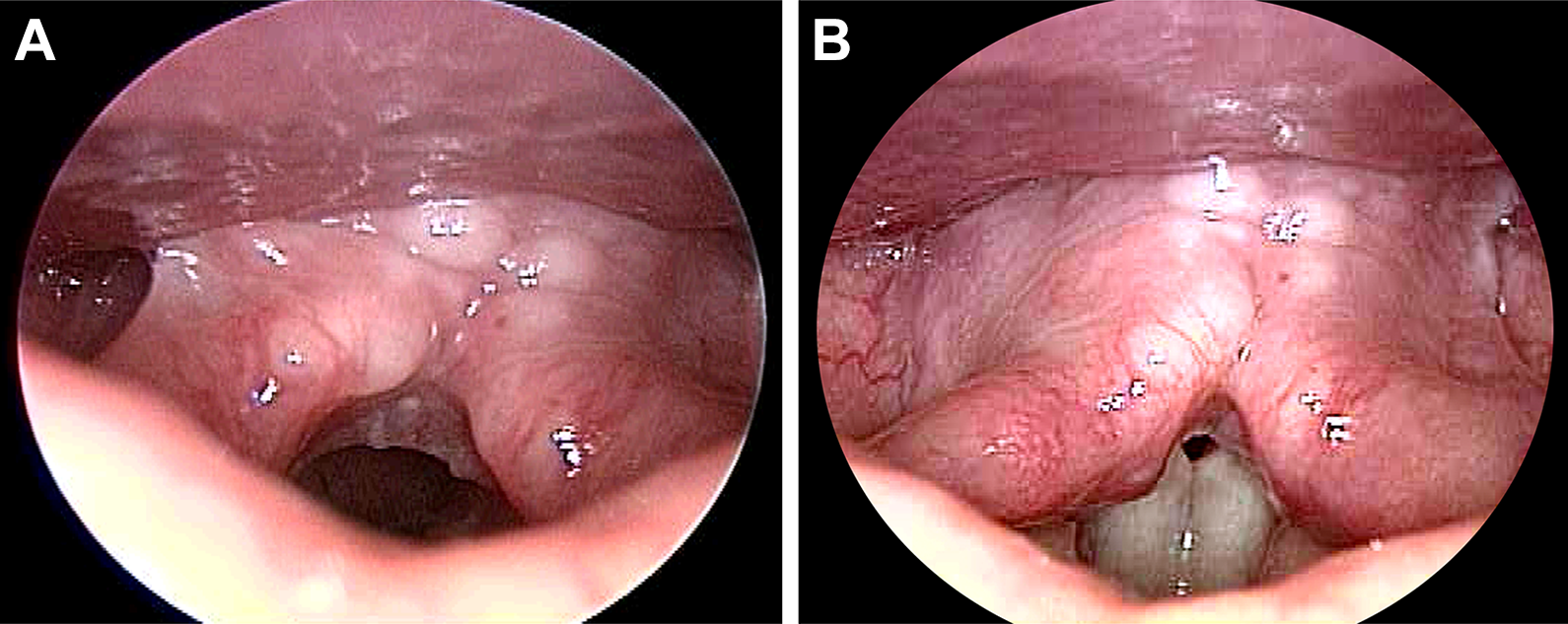
Laryngoscopy reveals multiple cobblestone-like pachydermia spreading across the interarytenoid and postcricoid regions during the vocal fold abduction (A) and phonatory adduction (B).
Laryngopharyngeal reflux has been recognized as an extraesophageal variation of GERD that occurs in up to 70% of patients with GERD. 1 Compared to gastroesophageal reflux, which is characterized by regurgitation, heartburn, and dyspepsia, the clinical presentations of LPR vary but may manifest as a globus sensation in the throat, hoarseness, frequent throat clearing, sore throat, cough, postnasal drip, a feeling of tightness in the throat or neck, and other symptoms. Some patients are asymptomatic. Both LPR and GERD are believed to result from dysfunction of the esophageal sphincters, and they can be distinguished as reflux that involves the upper esophagus, pharynx, and larynx (LPR) and reflux confined to the lower esophagus (GERD). However, the dysfunction of the upper esophageal sphincter (UES) is not the only etiology for LPR. Carbonic anhydrase, an enzyme known to protect mucosal tissues from acid contents, is expressed in significant quantities in normal laryngeal tissue but is absent in 64% of LPR patients. 2 Another cause of LPR is the heterotopic gastric mucosa of the esophagus, which is challenging to distinguish clinically from more common causes of LPR 3 but which usually can be diagnosed with esophagoscopy.
Laryngopharyngeal reflux can be associated with other disorders, including otitis media, sinus disease, Eustachian tube dysfunction, and obstructive sleep apnea. 4 By contrast, classic GERD is more strongly associated with Barrett’s esophagus and adenocarcinoma, although the prevalence of Barrett’s esophagus as high as 15.6% is reported in patients with pure LPR. 5 Some studies have indicated a higher prevalence of reflux disease in patients with laryngeal cancer, but this view still lacks strong evidence because of the confounding effects of smoking and alcohol consumption. 6
Monitoring with 24-hour dual pH probes can provide information pertaining to acid reflux. Multichannel intraluminal impedance/pH metry, which detects acid, weak acid, and nonacid reflux events, is more likely to provide a confirmation of LPR. Recently, Borges et al suggested that placement of the impedance electrodes above the UES to detect “pharyngeal reflux” could further facilitate the diagnosis of pathological LPR. 7 Nevertheless, in clinical practice across areas, a diagnosis of LRP was usually based on a combination of clinical symptoms and laryngoscopic findings. The cobblestone appearance on laryngoscopy reflects nodular lymphoid hyperplasia in response to inflammation or chronic irritation, such as in LPR in the present case.
Treatment of LPR should involve counseling on dietary and lifestyle changes, since behavioral changes can improve symptoms substantially. For example, Steward et al reported that 50% of patients had symptom improvement after behavioral changes, compared with 53% treated with a proton pump inhibitor (PPI). 8 The role of medication has been questioned, but PPIs remain the primary treatment and are effective for LPR signs and symptoms. 9 In addition, recent studies have revealed a high prevalence of nonacid or mixed refluxes, leading to a recommended addition of alginate or magaldrate to PPIs for suspected or confirmed LPR. 10 Our patient has achieved suppression of her symptoms after PPI treatment; however, the cobblestone appearance had changed little during her 10-year follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.