
Abstract
Background:
To demonstrate the efficacy of a new laser surgical technique for bilateral vocal fold immobility (BVFI) on postoperative quality of voice and swallowing.
Methods:
Prospective study in a tertiary university hospital and a private hospital. Patients with iatrogenic BVFI were included. Outcome measures were Voice Handicap Index 10, 10-item Eating Assessment Tool, flexible laryngoscopy, and success of decannulation.
Results:
Forty patients with post thyroidectomy BVFI were initially enrolled in our study; only 12 patients returned questionnaires and kept their follow-ups and were included in the study. All patients were successfully decannulated and remain decannulated up to 24-month follow-up. There was a statistically significant improvement in quality of swallowing and no significant deterioration in quality of voice. There was no need for revision up to 24-month follow up.
Conclusions:
The “Π” technique using diode laser technology is a new and safe technique for BVFI with excellent long-term decannulation rates and improvement in quality of life and swallowing without significant changes in voice quality.
Introduction
Posterior laser transverse cordotomy or Kashima’s operation has been shown to be an effective endoscopic procedure for bilateral vocal fold immobility (BVFI). 1 The main drawback of this procedure, when compared to more aggressive “glottic aperture improvement” operations, is the high revision rates, caused by granulations, adhesion, scar, and so on. 2,3 A recently published technique using diode laser appears to be a promising safe alternative for treating bilateral vocal fold palsies and minimizing revision rates. 4 The aim of this study was to prospectively assess the impact of this procedure on quality of voice and swallowing.
Methods
Forty patients with iatrogenic post thyroidectomy BVFI were included in the study. For the purposes of homogeneity, other noniatrogenic causes of BVFI, including idiopathic, were excluded. Patients who had previous failed “glottic aperture improvement procedures” in other institutions were also excluded. Patients who did not attend all scheduled 3 monthly follow-up appointments were also not included in the study. Complete symptomatic response was defined by the decannulation rates and the need or not for revision operation. Our main outcome measures were swallowing, assessed by the Eating Assessment Tool 10 (EAT-10), 5 and voice, assessed by Voice Handicap Index 10 (VHI-10). 6 Secondary outcome measures were the success of decannulation, flexible laryngoscopy, and the need or not for revision operations.
Operative Technique
The patients underwent the same technique as described below by the same surgeon (P.D.K.). The first part was a standard posterior transverse cordotomy. Laser precautions were implemented and the patients underwent general anesthesia through the tracheostomy tube. A microlaryngoscopy suspension system was used and a 980 nm diode laser flexible fiber was used through a laryngeal hand piece at 4 to 6 W continuous mode. The incision started from just anterior to the vocal process and extended laterally 3 to 4 mm into the false vocal fold. The resulting shape was a C-shape or a lateral Greek letter “Π.” 4
After this part of the procedure was completed, we inspected the area with a 0° or 30° rigid endoscope (Figure 1). Laser char was removed by rubbing a saline-soaked neuropatty. We then proceeded with the same diode laser flexible fiber and increased the settings at 8 to 9 W continuous mode (Figure 2). We directed the tip of the fiber into the deep part of the “Π” οr the “C” that we have created at the first part of the procedure. Multiple piercings of this area are done by inserting 5 mm of the fiber into the deep part of the original incision literally watching the tip of the laryngeal handpiece “near-touching” the larynx. The area was “deflated” as the tissue was vaporized after no more than 4 to 5 seconds and the fiber was withdrawn. Multiple piercings are done until we ensure the final “Π” result is flush with the lateral subglottic wall. At the end of procedure, we applied topical mitomycin C (0.4 mg/mL for 4 minutes).

Intraoperative picture of the cordotomy opening with the 980 nm diode laser fiber in place and an adrenaline-soaked neuropatty in place.
Diode laser settings.
Results
Twelve patients fulfilled our inclusion criteria. All patients were post total thyroidectomy, all done in other institutions. They all had emergency tracheostomies done by the local otolaryngologists immediately or within 72 hours after surgery and had no other “glottic aperture improvement” operations done since. When assessed by our team and recruited in the study, they were all at least 12 months post the iatrogenic insult with no signs of recovery. The male to female ratio was 1:4, and the ages ranged from 24 to 78 years (median, 56 years).
Eleven patients were decannulated in theater, and only one had to be decannulated 1 hour postoperatively in a high dependency unit as a precaution due to coexisting severe asthma. Decannulations remain successful up to 2 years, which is to date the longest follow-up. All patients filled voice questionnaire (VHI-10) before the operation and 1 month and 1 year after the operation and swallowing questionnaire (EAT-10) before and 2 years after the operation. Tables 1 and 2 summarize our results and show statistically significant improvement in swallowing and no significant change in voice 2 years postoperatively. The rest of the operated patients, although excluded from the study because of poor compliance with their follow-up appointments, had telephone assessments and remain well, tracheostomy-free, and did not have revision surgery for restenosis.
Voice Outcome 1 Month and 2 Years After the Π Technique for BVFI.a
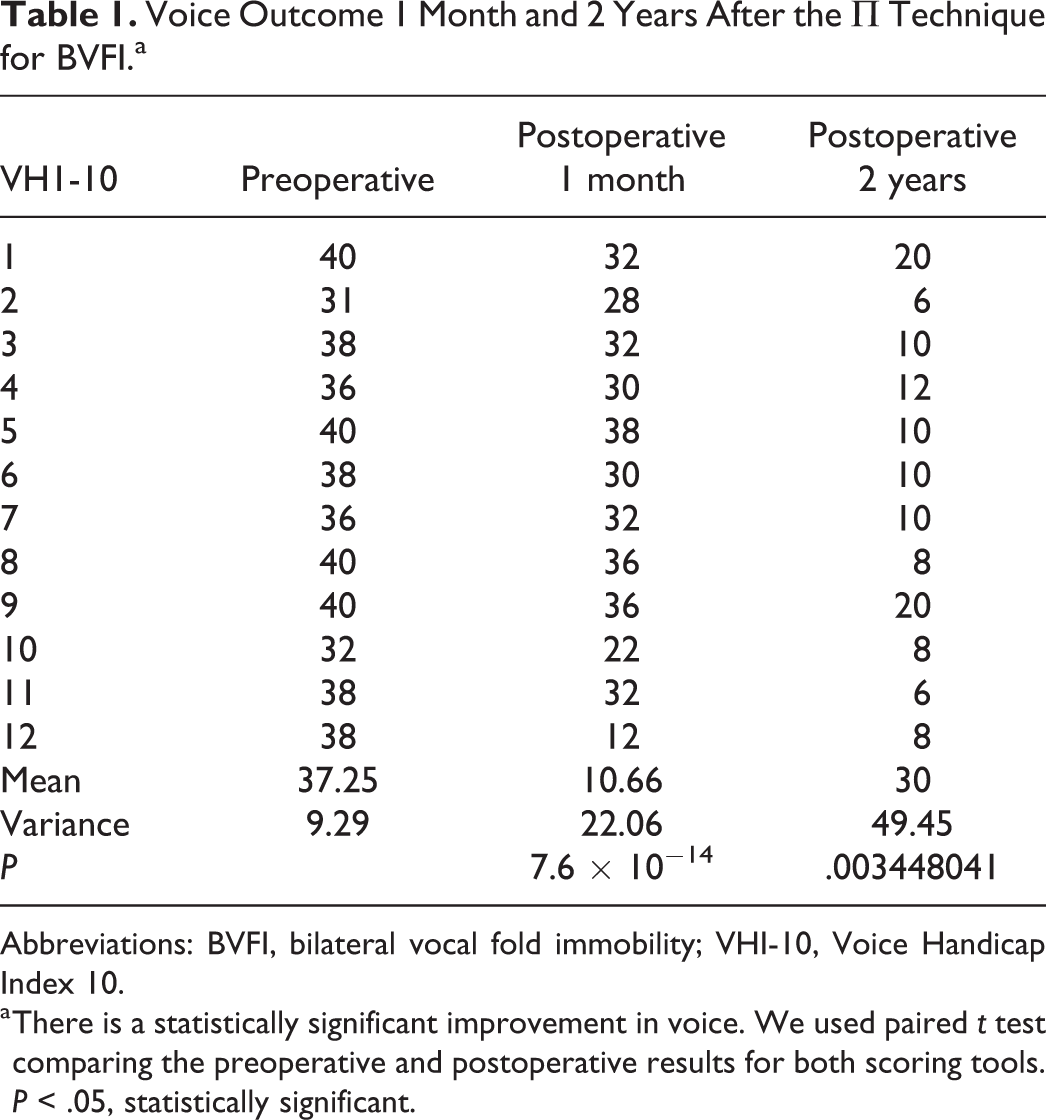
Abbreviations: BVFI, bilateral vocal fold immobility; VHI-10, Voice Handicap Index 10.
a There is a statistically significant improvement in voice. We used paired t test comparing the preoperative and postoperative results for both scoring tools. P < .05, statistically significant.
Swallowing Outcome 2 Years After the Π Technique for BVFI.a
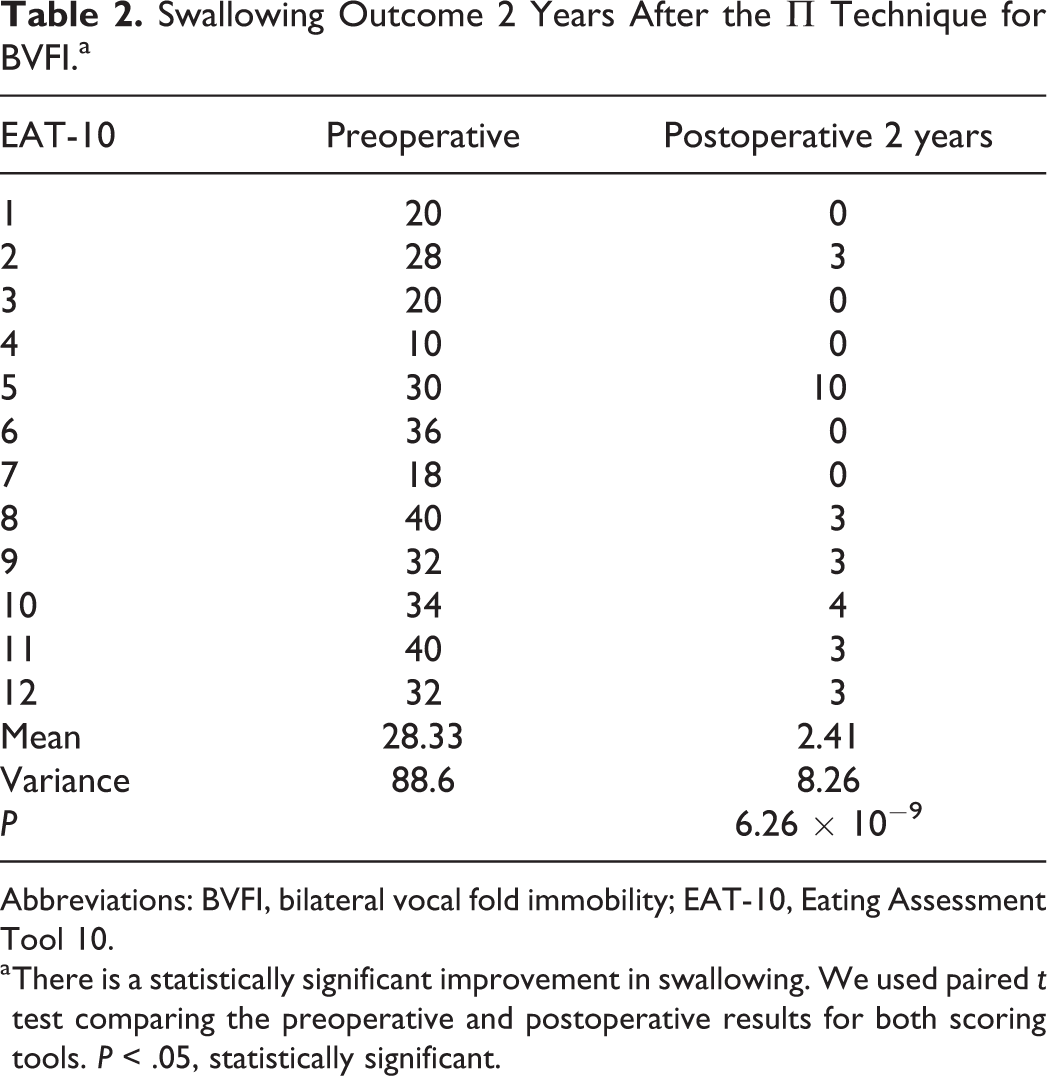
Abbreviations: BVFI, bilateral vocal fold immobility; EAT-10, Eating Assessment Tool 10.
a There is a statistically significant improvement in swallowing. We used paired t test comparing the preoperative and postoperative results for both scoring tools. P < .05, statistically significant.
Discussion
It is a well-known fact that quality of life, voice, and swallowing are affected after a tracheostomy irrespective of the reason behind it. 7,8 There is also a significant impact on psychological well-being and self-image in tracheostomized patients. 9 Bearing in mind that a significant amount of patients undergoing thyroid surgery (the commonest iatrogenic cause of BVFI) are young or middle aged, 10 the impact of waking up with a tracheostomy, in the event of a BVFI, is undoubtedly severe.
Experience has shown that “glottic aperture improvement procedures” can successfully help patients be decannulated but have a negative impact on quality of voice. 11,12 Unilateral laser cordotomy as opposed to bilateral cordotomy or the more aggressive arytenoidectomy is a minimally invasive operation that appears to be safe for BVFI. This is the first study to our knowledge that shows as expected—since all patients were successfully decannulated—improvement in swallowing but more importantly no voice deterioration at least 18 months after surgery with no need for revision and/or more aggressive glottic procedures.
It seems that diode laser, especially for the more “lateral” part of the cordotomy, may have a less detrimental effect on the tissues and therefore a less adverse effect on voice, although this remains to be further proven with a histological study. There is not a lot of evidence in the literature regarding the use of diode laser in laryngeal surgery. The diode laser emits wavelengths that are absorbed by hemoglobin and melanin, and because the penetration depth depends on these chromophores, these properties make it an ideal tool for photocoagulation. 13 The surgical precision of diode laser may be slightly inferior to CO2 but has a superior coagulation capability. 14 Additionally, diode laser’s beam can be carried through flexible optic fibers, reaching difficult to explore sites, such as very lateral glottic and subglottic regions. And even though CO2 can over recent years be also delivered through flexible hollow tube, the use of diode laser by contact or near-contact makes it safer than other lasers by avoiding collateral damage due to “beam scape” in an open field. 13,14
Conclusions
The “Π” technique using the 980 nm diode laser appears to be safe and “friendly” to the voice technique for iatrogenic BVFI with excellent long-term decannulation rates and no significant deterioration in voice quality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.