
Abstract

A 56-year-old male presented with right-sided aural fullness and otorrhea for 1 month. He denied past history of trauma, hearing loss, vertigo, or otitis media. Otoscopic examination demonstrated a wide-based, grey-purple-colored, and hard mass occupying nearly the right external auditory canal (EAC; Figure 1A). The audiogram showed symmetric hearing without conductive hearing loss. High resolution computed tomography of the temporal bone revealed one soft tissue lesion with calcified spots along the posterosuperior wall of the right EAC (Figure 1C and D). We excised the tumor totally via endaural approach by microscopy under general anesthesia (Figure 1B). Histopathologic evaluation demonstrated small and large dilated vessels that were lined by endothelial cells filled in fibroblastic and collagenous stroma, and the lumina contained sporadic blood cells by hematoxylin and eosin staining (Figure 2A). Immunohistochemical staining with CD34 (Figure 2B) and CD31 (Figure 2C) were positive for endothelial cells of microvessels. In our patient, no blood cell components were noted with positive D2-40 expression for lymphatic vessels (Figure 2D). Based on immunohistologic findings, the diagnosis was compatible with capillary lymphangioma. The wound was healed spontaneously and no evidence of recurrence in the follow-up.
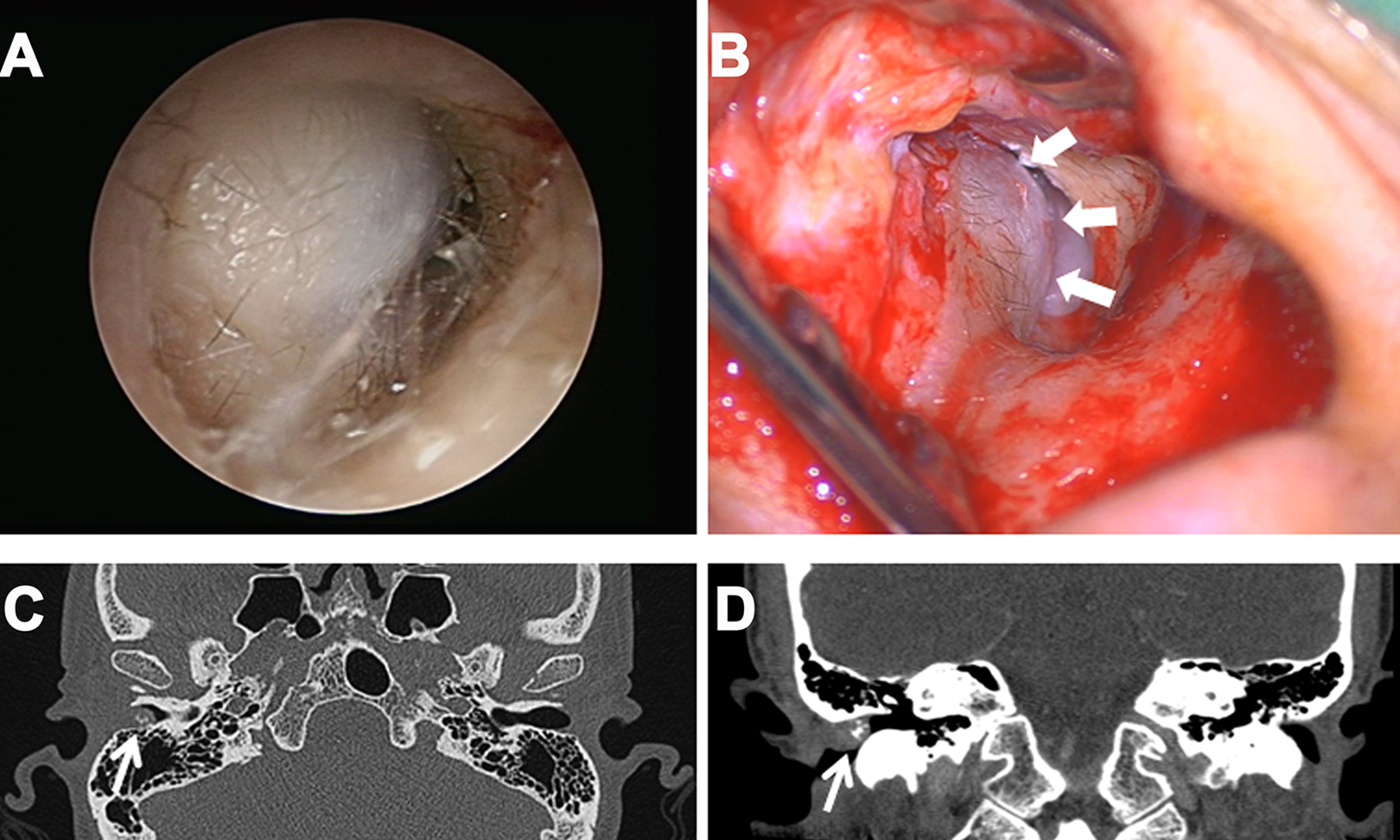
(A) The otoscopy showed a grey-purple colored, tender and hard mass occupying nearly the right external auditory canal (EAC). (B) The surgical excision of the tumor (arrows) was via endaural approach. High resolution computed tomography of the temporal bone demonstrated a 10 × 10 × 5 mm lesion (arrow) with calcified spots in the posterosuperior wall of right EAC with mild bone erosion in axial view (C) and coronal view (D).
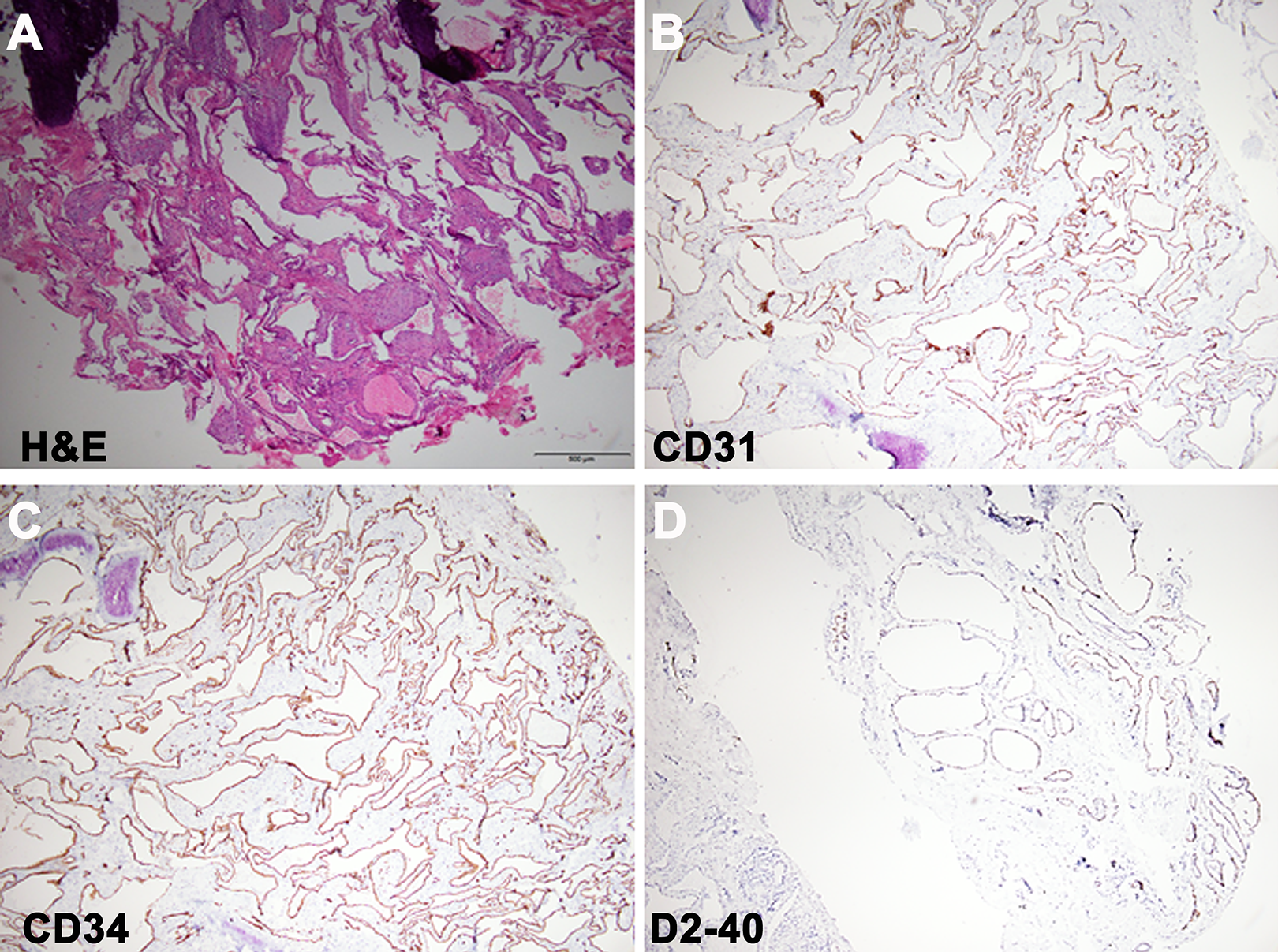
(A) Microscopically, the specimen showed the irregular dilated vessels lined by flattened, bland epithelial cell filled in fibroblastic and collagenous stroma with some hemosiderin deposition with positive CD31 (B) and CD34 (C) expression. (D) D2-40 stain expression was positive for lymphatic channels. Scar bar = 500 um in all fields.
Lymphangioma, also known as lymphatic malformation, is a benign, hamartomatous tumor of the lymphatic system, which may be congenital or acquired. Acquired lymphatic malformations may result from infection, trauma, or chronic lymphatic compression. 1 It occurs in the head and neck region with up to 70%, which the most common location is the submandibular region, followed by the parotid gland.2,3 Its occurrence in the EAC is very rare. 4
Lymphangiomas have been classified into 3 types by the diameter of the vessels: (1) capillary lymphangioma, consisting of small, capillary-sized vessels; (2) cavernous lymphangioma, comprising large, dilated lymphatic vessels; and (3) cystic lymphangioma exhibiting large macroscopic cystic spaces. 5 Histopathology revealed lymphatic vessels lined by attenuated endothelium with marked dilatations which may be empty or appear consist of proteinaceous material and occasional blood cells.
The differential diagnosis should be inclusive of hemangioma, which is histopathologically similar to lymphangioma. 6 Immunohistochemical staining with CD31 and CD34 are generally used for identification of microvessels, but not specific for lymphatic vessels. D2-40, a monoclonal antibody, can be used as a reliable marker to differentiate lymphatic vessels from blood vessels by identifying an oncofetal glycoprotein which was found in lymphatic endothelial cells but not in blood endothelial cells. 7 Imaging of lymphangioma in the temporal bone is reported to be accompanied by bone destruction as our presented case. 6
The treatment of lymphangioma include observation, aspiration, injection, cryotherapy, electrocautery, radiation, laser, ligation, and excision depending on the size of the lesion, localization, and complications. 8
To our knowledge, this is the first report of lymphangioma involving the EAC presented in the English literature. Although EAC lymphangioma is rare and benign, it could cause patient’s discomfort and conductive hearing loss; thus, warrant early recognition and management.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-D-109053 to H.-C. Chen).