
Abstract
Objectives:
A wide and evolving range of lasers and their applications often makes it difficult for a busy surgeon to choose the ideal laser for a specific indication. With this in mind, this article aims to summarize the most recent literature concerning laser application in rhinology.
Methods:
A literature search from 2000 to 2020 using the PubMed database was employed. Keywords used included “laser,” “rhinology,” “endonasal endoscopic surgery,” “hereditary haemorrhagic telangiectasia,” “rhinitis,” “refractory rhinitis,” “Inferior turbinate hypertrophy,” “dacryocystorhinostomy,” “septoplasty,” “cartilage reshaping” and “choanal atresia.” The most up to date studies published for each rhinology condition that could potentially be treated with laser surgery was included.
Results:
Rhinological conditions appropriate for laser applications are discussed. We identified articles related to a number of applications including hereditary hemorrhagic telangiectasia, rhinitis, turbinate surgery, dacryocystorhinostomy, septoplasty, choanal atresia, and sphenopalatine artery ligation, paying attention to the outcomes of the studies and their limitations.
Conclusions:
There is currently no one-size-fits-all laser and therefore being up to date on the latest clinical application results can help the clinician decide which are the best treatments to offer their patients.
Introduction
Light amplification by stimulated emission of radiation (Laser) was first described by Maiman in 1960. 1 Over the next 60 years, the development of different types of lasers has allowed for a variety of clinical applications of lasers to treat a range of diseases. Laser surgery has assumed a key position in minimally invasive treatment concepts in almost all areas of otorhinolaryngology.
The common types of lasers that used in the subspecialty of rhinology include argon (Ar), potassium titanyl phosphate (KTP), diode, neodymium-doped yttrium aluminum garnet (Nd: YAG), holmium-doped yttrium aluminum garnet (Ho: YAG), and the most popular carbon dioxide (CO2). Each laser type has different properties for cutting, coagulation, and evaporating of tissues. The delivery system also varies, with contact and noncontact methods possible. A wide and evolving range of lasers and their applications often makes it difficult for a busy surgeon to choose the ideal laser for a specific indication. With this in mind, this article aims to summarize the most recent literature concerning laser application in rhinology.
Methodology
A literature search from 2000 to 2020 using the PubMed database was employed. Keywords used included “laser,” “rhinology,” “endonasal endoscopic surgery,” “hereditary haemorrhagic telangiectasia,” “rhinitis,” “refractory rhinitis,” “Inferior turbinate hypertrophy,” “dacryocystorhinostomy,” “septoplasty,” “cartilage reshaping,” and “choanal atresia.” The most up to date studies published for each rhinology condition that could potentially be treated with laser surgery was included.
Summary of Lasers and Their Properties
It is important for the clinician to understand the interaction between laser radiation and tissues and to be aware of the main technical parameters of the lasers that they choose to use clinically. Table 1 shows a summary of the properties of different laser systems commonly used in rhinology surgery. 2
Summary of Lasers and their Properties.
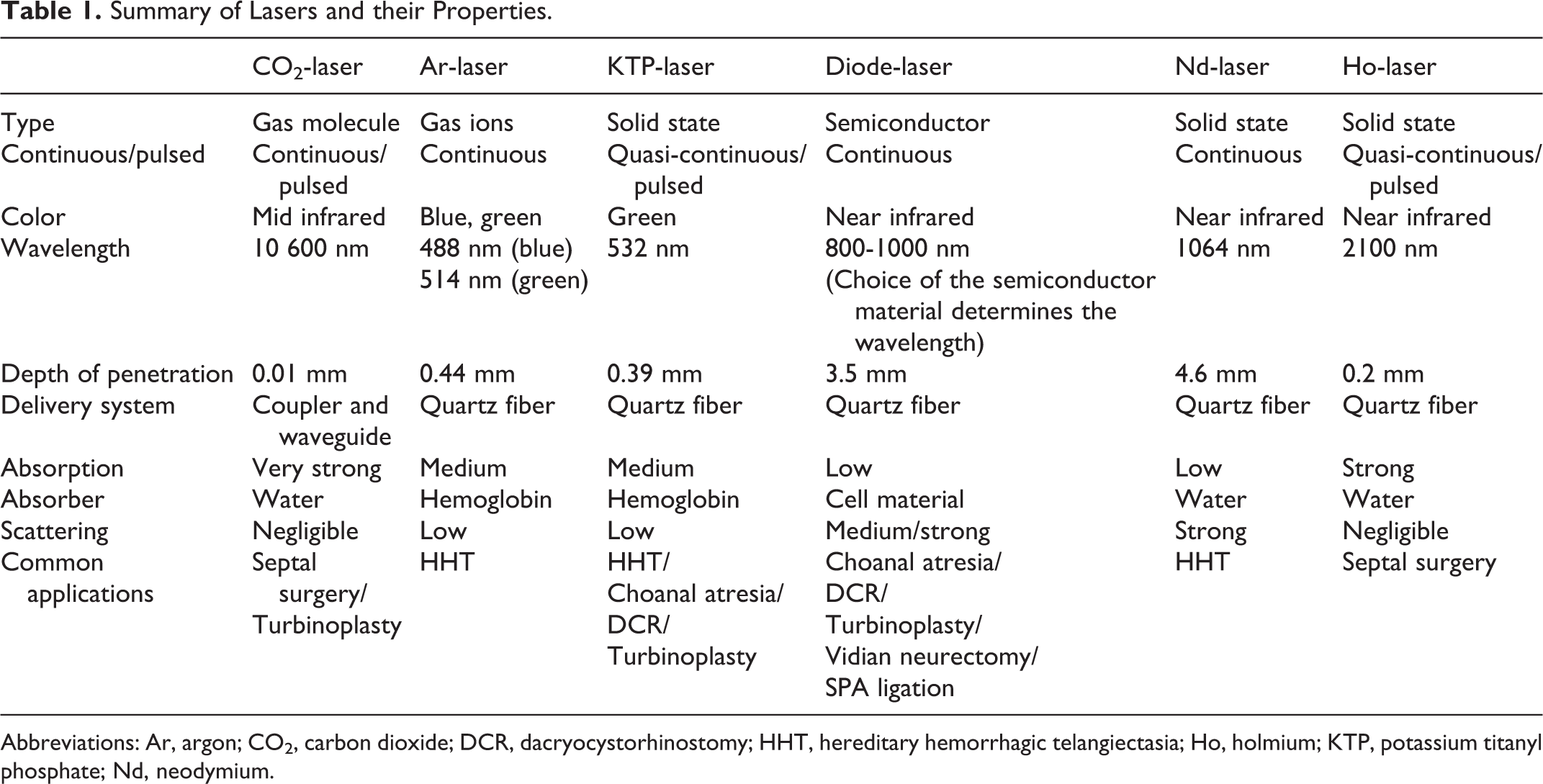
Abbreviations: Ar, argon; CO2, carbon dioxide; DCR, dacryocystorhinostomy; HHT, hereditary hemorrhagic telangiectasia; Ho, holmium; KTP, potassium titanyl phosphate; Nd, neodymium.
Rhinological Conditions Appropriate for Laser Applications
Hereditary Hemorrhagic Telangiectasia
Hereditary hemorrhagic telangiectasia (HHT) or Osler–Weber–Rendu disease is an inherited autosomal dominant vascular disorder and most commonly manifests to the otolaryngology department with epistaxis. A 2020 systematic review 3 which included 362 patients discussed the efficacies of the three most common laser photocoagulation treatments for HHT-related epistaxis—these included Ar, Nd: YAG, and diode. The lasers’ efficacies were evaluated by reduction in rates of epistaxis frequency and intensity. Potassium titanyl phosphate operates at a similar green wavelength (like the Ar laser), enabling it to be specifically absorbed by haemoglobin. 2 However, despite its growing prominence in epistaxis treatment, there are limited number of studies that have evaluated its efficacy in improving epistaxis outcomes in HHT patients. 4 The results revealed that intranasal laser photocoagulation of telangiectasias using Ar or Nd: YAG laser therapy can yield improved epistaxis outcomes compared with diode. In severe cases of HHT, Nd: YAG laser therapy provides greater improvements in epistaxis outcomes than Ar photocoagulation. 2
Rhinitis (Without Polyps)
Rhinitis is a condition which involves inflammation of the nasal cavity. The initial treatment of rhinitis or rhinosinusitis is mainly medical with a combination of topical or systemic agents such as steroids and antihistamines. 5 Since described in the 1960s, vidian nerve (VN) neurectomy paved the way to surgical therapy for refractory rhinitis. 6 Since then, posterior nasal nerve (PNN) surgery has also been described as alternative treatment for allergic and vasomotor rhinitis.
A study in 2017 compared results from 118 patients who underwent diode laser-assisted versus traditional VN neurectomy. 7 Vidian nerve was excised with a 940-nm continuous wave (CW) diode laser through a 600-µm silica optical fiber, utilizing a contact mode with the power set at 5 W. Changes in the visual analogue scale (VAS) were significant in preoperative and postoperative nasal symptoms in both groups. The application of diode lasers for VN transection showed a better surgical field and a lower incidence of postoperative hemorrhage. There was no mention of any carotid injury, but 2.3% of the group of patients who underwent diode laser-assisted neurectomy had cheek numbness (comparable to the 2.6% in the group who had a traditional cold instrument neurectomy). The authors therefore advocate the diode laser-assisted endoscopic intrasphenoidal approach, especially for patients with vidian canal protrusion.
More recently, Krespi et al 8 described the endoscopic diode laser ablation of the PNN. Using a 940 nm diode laser with a 400-micron uninitiated malleable fiber tip, the PNN region was ablated using a CW at a power setting of 5 W in a noncontact mode for about 10 to 15 seconds. Pain scores were low, and there were minimal postoperative side effects. Results from 32 patients showed the procedure to be safe and well tolerated both in the office and ambulatory settings. Symptom scores were significantly decreased after 30 and 90 days.
Turbinate Surgery
Allergic inferior turbinate hypertrophy is a common cause of nasal obstruction. The management of allergic rhinitis is initially medical but a surgical approach sometimes becomes necessary when medications fail. 5 Presently, there is a lack of consensus as to the ideal surgical mode of treatment for turbinate hypertrophy; however, the consensus is that techniques which preserve nasal mucosa have lesser side effects and complications than those techniques in which the mucosa is damaged. 9 Laser turbinate reduction has the advantage of reduced bleeding, high precision, less intraoperative time, and good healing of the wound. 10
A recent study from 2016 11 studied 30 patients for the efficacy of KTP laser turbinate reduction in terms of symptomatic improvement and its effect on nasal mucociliary clearance. All procedures were carried out as an outpatient procedure under local anesthetic. Potassium titanyl phosphate laser parameters were set to 6 W at continuous mode and energy delivered through an optical fiber. The laser tip was held at contact mode with the mucosa surface and 4 to 5 passes were made along the surface of inferior turbinate in an anterior to posterior direction. The mean duration of the procedure was 12 minutes. There were no major complications, but the most common patient complaint noted in the early postoperative period was crusting. Although nasal mucociliary clearance was temporarily impaired in the initial postoperative period, it returned to normal thereafter. There was also significant improvement in the sino-nasal outcome test post operatively up to 3 months. Techniques vary between groups with some groups preferring to use a submucosal application rather than on mucosa, but in general these studies have similar positive results in reducing symptoms. 12 -17
A great variety of CO2 laser surgical techniques for turbinate surgery is described in the literature. Selkin 18 previously used the CO2 laser sighted through a surgical microscope to resect the hypertrophied mucosa of the turbinate, whereas Elwany and Harrison 19 and Englender 10 vaporized the mucosa in the anterior one-third of the turbinate (also through a surgical microscope). Fukutake et al 20 in 1986 20 removed the entire mucosa of the inferior turbinates by evaporization (using a specialized handpiece for straight and reflected CO2 laser beam), once in a week for 5 weeks. However, as mentioned previously, techniques which preserve nasal mucosa tend to be preferred and recently Hussain and Ahmad 21 published results from spot ablation of inferior turbinates. The study compared the subjective improvement of nasal obstruction before and after surgery using the nasal obstruction symptom evaluation scale (NOSE) and the VAS. The improvement in NOSE and VAS scores was statistically significant. There was also minimal postoperative pain and intranasal crusting. Similar results were also observed by Prokopakis et al 22 (the CO2 laser sighted through a surgical microscope) who noted a significant improvement in VAS scores for nasal obstruction postoperatively following CO2 laser turbinoplasty.
The diode laser is one of the most portable and least expensive of the lasers available for turbinate surgery and results from Cakli et al 23 in 2012 showed that mean operation time was 3 minutes per turbinate and there were no major complications. Both subjective and objective evaluations showed significant improvement with improved VAS scores and acoustic rhinometry measurements increased significantly 1 year after surgery. More recently, Doreyawar et al 24 compared outcomes by diode laser turbinate reduction and conventional partial inferior turbinectomy and showed that compared to the conventional technique, the outcomes were better with diode laser and caused less morbidity.
A study in 2007 by Sroka et al 25 compared the Ho: YAG with diode lasers. Both techniques resulted in statistically significant improvement in nasal airflow at 6 months and 3 years postoperatively, although the diode laser demonstrated a decline in airflow between 6 months and 3 years. They therefore concluded that the Ho: YAG laser had better long-term nasal patency compared with the diode. There are however no other studies comparing different types of laser surgery to each other.
Dacryocystorhinostomy
Dacryocystorhinostomy (DCR) involves creating a permanent surgical anastomosis between the lacrimal sac and the nasal cavity to overcome a lacrimal duct obstruction. Dacryocystorhinostomy can be carried out via external incision or endoscopic techniques such as mechanical transnasal endoscopic DCR and transcanalicular laser DCR. Dacryocystorhinostomy was first reported by Toti 26 in 1904 via an external approach, but since then the methods have been refined and with the use of endoscopes, the endonasal approach is now commonly used. The advantages of endoscopic DCR are that it is less invasive, has a shorter operation time, preserves lacrimal pump function, has faster recovery, and avoids external scar. 27 Existing data are inadequate to draw conclusions about whether endonasal DCR is superior to, equivalent to, or inferior to the gold standard external DCR. 28 Laser-assisted DCR was first introduced in 1990 by Massaro et al 29 who used an Ar laser device and the operating microscope. Later on, other lasers including CO2, KTP, Nd: YAG, and Ho: YAG were described.
A retrospective study in 2019 looked at 596 patients who underwent transnasal endoscopic DCR over a 30-year period. Patients’ demographics and surgical techniques were assessed. Patients who failed revision DCR tended to be younger and more likely to have had intraoperative laser usage for the bone removal technique. 30 In contrast, another retrospective analysis of 423 patients 31 looked at the different surgical techniques and outcome. Comparing standard endoscopic DCR, endoscopic DCR with stent, endoscopic DCR with mitomycin C, powered DCR, KTP laser-assisted DCR (setting of 5 W for mucosa and 10 W for bone), and balloon DCR, there was no statistically significant difference in success rates, recurrences, or complications of various techniques at 3 or 6 months.
Diode laser-assisted transcanalicular DCR is highly topical and has featured in several recent papers internationally. Success rates have been quoted to be between 58% and 88%. 32 -34
Comparing external DCR with laser-assisted transcanalicular DCR, Hong et al found that the success rate for external was 90% to 95% compare to 82.4% for transcanalicular DCR. 33 Recently, some data were published comparing results from mechanical transnasal endoscopic DCR versus transcanalicular multidiode laser DCR. 27 Complete resolution was achieved in mechanical transnasal endoscopic DCR, whereas failures stemming from canalicular stenosis and fibrosis at osteotomy site were recorded in 2 cases in transcanalicular multidiode laser DCR group (each group had 15 patients).
Septoplasty (Including Cartilage Shaping)
Nasal septal medialization surgery in the form of submucous nasal cartilage resection or septoplasty is a common operation performed in otolaryngology. In 2000, Kamami et al 35 described a novel 5-minute procedure using CO2 laser to ablate the anterior septal spur under local anesthetic. A CO2 laser on super-pulse continuous mode on 10 W was used. The inferior turbinate was partially resected in all cases as well. Results were reported from 703 patients who were followed up for a mean length of 12 months. There was a 1.7% rate of mild epistaxis postoperatively and 0.7% of patients developed nasal adhesions which were treated with a subsequent CO2 laser treatment. There were no recurrent septal deviations or septal perforations. There were also improvements in patient reported outcome measures as well as acoustic rhinometry.
A study in 2010 36 tried to overcome the limitations of the CO2 laser handpiece by using a more maneuverable diode laser fiber. This also allowed the authors to address even the posterior spurs under the endoscopic view. The study reports results from 1000 patients of which the CO2 laser was used on 700 patients and the diode laser on 300. A similar setting of the CO2 laser as used in the Kamami et al 35 paper was used. The diode laser was operated in a continuous mode at 6 W and connected to a 300-μ bare and flexible fiber inserted to a specially designed handpiece. The diode laser has to be activated in contact mode for effective tissue ablation unlike the CO2 laser. The NOSE questionnaire was used to evaluate patient’s satisfaction and only in some patients were the acoustic rhinometry done. The presented results did not compare the CO2 to the diode, but in general patient satisfaction was 96%. There were no septal perforations, minor bleeding occurred in 0.8% and 0.7% developed synechia requiring secondary correction.
While the techniques described above is potentially useful in patients with septal spurs, it does not address a large number of patients who have C-shaped cartilage deviations.
Bourolias et al 37 in 2008 evaluated the results from septal cartilage reshaping with the use of an Erbium doped glass fiber laser under local anesthetic. The authors explain that the ideal indication for this procedure includes C-shape septal cartilage deviation and minimal cartilage deviation after septal surgery and is useless with any bony deviations. An Erbium-doped glass fiber laser at a wavelength of 1.56 µm and power of 4.1 W was used. The cartilage of nasal septum was straightened and fixed in the median position using a modified nasal speculum. An optothermomechanical contactor with transparent indenter and thermocouple sensor was placed on septal regions of maximum mechanical stress. Results from 64 patients showed statistically significant improvement of their symptoms and of rhinomanometric results. No complications or side effects occurred. Results from Leclère et al 38 in 2010 were similar.
A similar study was performed with use of a Ho: YAG Laser in 110 patients. 39 The average duration of follow-up was 18 months. Eighty-four (76%) patients showed stable improvement in nasal obstruction and disappearance of the attendant symptoms.
Choanal Atresia
Choanal atresia may be unilateral, or bilateral, and may be due to persistent tissue which is bony, membranous, or most commonly a combination of both. Traditional surgical approaches include the transnasal, the transseptal, and the transpalatine, but most surgery today is performed via the endoscopic transnasal approach using endoscopic instruments, and possibly a drill or a microdebrider. 40,41 Laser techniques have also been described.
Pototschnig et al 42 described using the KTP laser in 13 patients with the laser employed with a fiber in a slim handpiece in contact mode. A setting of 3 to 5 W in continuous mode was used. The operation was performed under direct vision with the assistance of a 30° angled endoscope. In all cases, an intranasal stent was inserted. There were no complications with wound healing and in all cases, there were no intraoperative complications and no postoperative bleeding. Follow-up was up to 3.5 years and one patient had some granulations that were easily removed but there were no cases of restenosis. In the same year Tzifa and Skinner 43 described the transnasal endoscopic repair with the KTP laser without stenting. Three patients with unilateral choanal atresia were treated. Follow-up was between 1 and 4 years with no cases of restenosis. No surgical complications were reported.
Hopf et al 40 described the transoral retropalatine approach for endoscopic fiber-guided diode laser surgery of choanal atresia. The results from 5 patients were presented, and in all cases, a stent was inserted. Technically, the mucosa is prepared first with a superficial coagulation with the diode laser on continuous, noncontact mode at 2 to 5 W. Then dissection of the bony atresia plate by vaporization occurs on pulsed, contact mode at 12 to 50 W. The outcome and follow-up showed good results concerning wound healing with no complications or restenosis. D’Eredità and Lens 41 a few years later also described using the fiber-delivered contact-diode laser in 4 low-weight newborns. Two patients did require revision surgery but the authors pointed out that while non-laser surgical approaches are an option, instrumentation can be difficult to place with the narrow newborn nasal vault, particularly in low-birth weight neonates. Therefore fiber-delivered laser approach allows surgery to occur within such confines.
The literature is full of the experiences of a number of authors with no randomized control trials. There is no obvious single standard method of using a particular laser system, with or without stenting, that can be recommended in order to achieve good long-term results getting no restenosis.
Sphenopalatine Artery Ligation
Epistaxis is a common otolaryngological emergency and it has been reported that 5% to 15% of patients admitted to hospital will require surgical management, especially in the setting of posterior epistaxis. 44 -46 Endoscopic endonasal ligation of the sphenopalatine artery (SPA) was first described in 1992 and since then has become a popular choice for surgical control of posterior epistaxis. Normally clips, bipolar diathermy or a combination of both is used to ligate the SPA. 47
Recently a group from Greece described the technique of a flexible diode-laser SPA ligation as an alternative to the classic approach (clips or diathermy). 48 Flexible 980 nm Diode laser fiber was used through a nasal or laryngeal handpiece in a near-contact mode to the SPA at energy of 5 to 7 W for 5 seconds in a CW where access to the SPA area was limited due to septal spurs, very narrow nose, or significant bleeding. Surgical time was kept under 60 minutes and there were no reports of rebleed or other complications. However, only 3 cases were described and so while this method may seem promising as it appears safe and quick, certainly additional studies need to be undertaken to examine this technique further.
Discussion
The ideal laser for rhinology needs to efficiently ablate dense bone, remove soft tissue, and coagulate a dense vascular bed. There is currently no one-size-fits-all laser, and hence, it is important for the clinician to be aware of their basic technical properties and have some knowledge as to which laser has the sufficient depth of penetration to remove tissue while preserving and protecting the underlying important structures. Being up to date on the latest clinical application results can also help the clinician decide, which are the best treatments to offer their patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.