
Abstract

The Bonebridge (BB; Med-El) is an active semi-implantable transcutaneous bone conduction hearing device which is implanted subcutaneously. 1 Its transcutaneous nature lends it the advantage of obviating skin aftercare, although gain might be slightly reduced in comparison to percutaneous devices due to the skin attenuation.1,2 It can be considered for adults, but successful implantations in children and adolescents have been also reported. 3 The implantation procedure can be challenging because of the bulk of the device’s large Floating Mass Transducer which needs to be accommodated in the confines of the mastoid cavity for ideal sound transmission. More specifically, the dimensions are 8.7 mm in thickness, 15.8 mm in diameter, and 23.8 mm between anchor holes.1,2 This is often difficult to fit within a mastoid cavity without significantly exposing and indenting either middle or posterior fossa dura or the sigmoid sinus. This is not preferred by many middle ear surgeons without neurotology experience or backup. Preoperative 3D image planning based on computed tomography (CT) scans and manual reformatting and measurements of bone thickness helps in assessing the ideal location without risking perioperative injury to vital structures. The manufacturer provides a 3D planning software to support this process. The 3D Labs software that we use locally, allows easier planning and has largely automated the process.
In our department, 16 patients were assessed for BB implantation and 15 were eventually implanted, one of them receiving bilateral implants. For our preoperative planning for implant position, we used the above software to virtually test the “ideal placement” of the implant at different sites (mastoid, retrosigmoid, etc) and evaluate the bone thickness and the distance from the other important anatomical structures. The 3D preplanning reduced surgical time by over 25% and surgical risks by eliminating the need for trial and error, giving the surgical team more confidence at surgery. One of the patients was found inappropriate for implantation due to an atretic mastoid bone and consequently received a BAHA instead (Figure 1). The preplanning predictions had a 100% match with the eventual surgical placements so that 5 patients had retrosigmoid implantation and the remaining had mastoid placements, with uneventful surgery and postoperative recovery. Figures 2 and 3 demonstrate successful preoperative planning, allowing implantation. The patient with bilateral implants had them done simultaneously without any further problems.
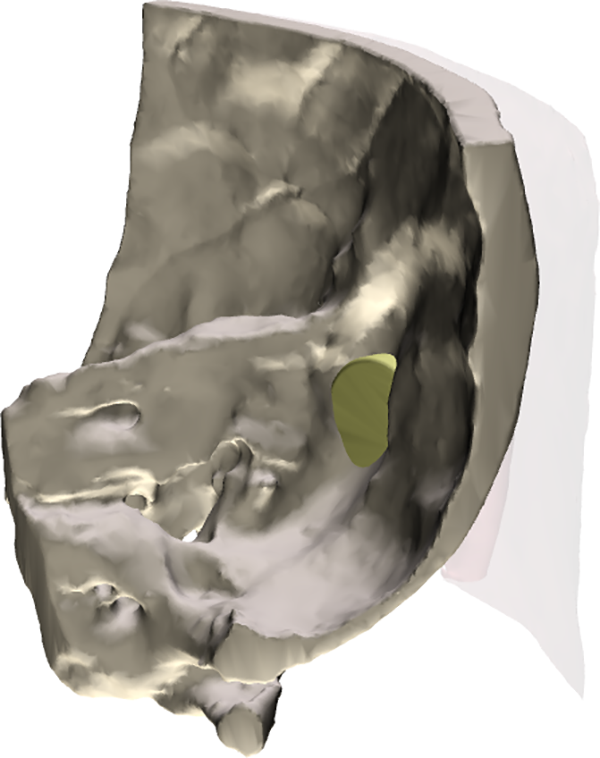
Preoperative planning failed as the implant is extending beyond the interior table of the temporal bone.
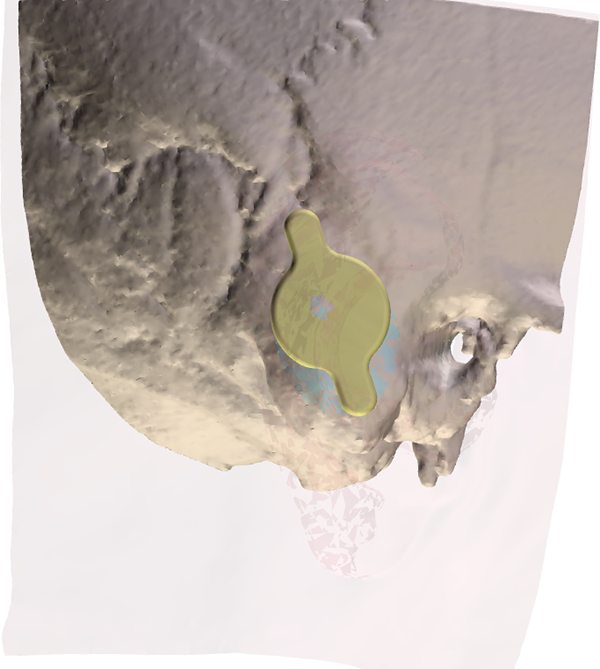
Preoperative planning—good candidate for implantation.
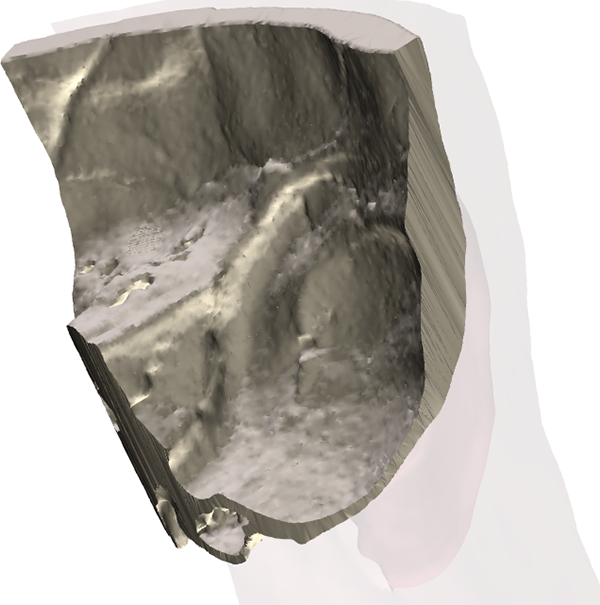
Preoperative planning—good candidate for implantation.
Several methods for preoperative planning have been reported in the literature. Canzi et al described the use of 3D printed skull models based on CT scans of the patients. They reported successful positioning on all human temporal bones, with a mean error of 0.13 mm. 4 Wimmer et al applied a topographic bone thickness map in the preoperative planning in 7 cases, although the thickness map was only radiologically elaborated and required the identification of anatomical landmarks to detect the BB location on patients. 5 Other studies have reported methodologies on producing 3D templated for identifying the BB positioning, which had previously been planned on the CT scan.6-9 Mukherjee et al reproduced 16 3D-printed models prior to implantation. They compared them with the standard assessment recommended by the manufacturer and concluded that there is statistically significant benefit in using 3D printed models to plan surgery in difficult cases. 10 Our technique of virtual 3D preplanning achieved all the benefits of the above principles without additional time or steps or the need for any consumables.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.