
Abstract

A 4-year-old female with no significant past medical history presented to the pediatric-ENT clinic for left-sided neck mass. The patient’s mother referred that when the patient came home from the school, she noticed a swelling to the left side of the patient’s neck. The patient stated that her younger 2-year-old sister kicked her in the neck the day before. There are no other reports of bug bites or neck abnormalities noticed at birth. The patient’s mother denied recent fevers or difficulties with breathing or swallowing. Flu antibodies and strep A screens were negative. Physical examination revealed a mobile, nonerythematous, nontender left neck mass. Ultrasound (US) of the neck was requested with concern for hematoma (Figure 1). Due to evidence of active bleeding in the US, a computed tomography (CT) angiography of the neck was performed, resulting in a challenging diagnosis of brachial cleft cyst versus lymphangioma. Magnetic resonance imaging (MRI) of the neck revealed hematocrit effect suggesting complex mass with hematoma (Figure 2). Neurointerventional radiology was consulted and the left neck mass was drained. Fine needle aspiration cytology reported blood with numerous lymphocytes corresponding to lymphangioma complicated by hemorrhage. The pediatric-ENT team and the patient’s mother agreed to provide expectant management and close monitoring to the patient’s condition. In follow-up clinic appointments, the patient’s left-sided neck mass decreased significantly in a 3-month period.
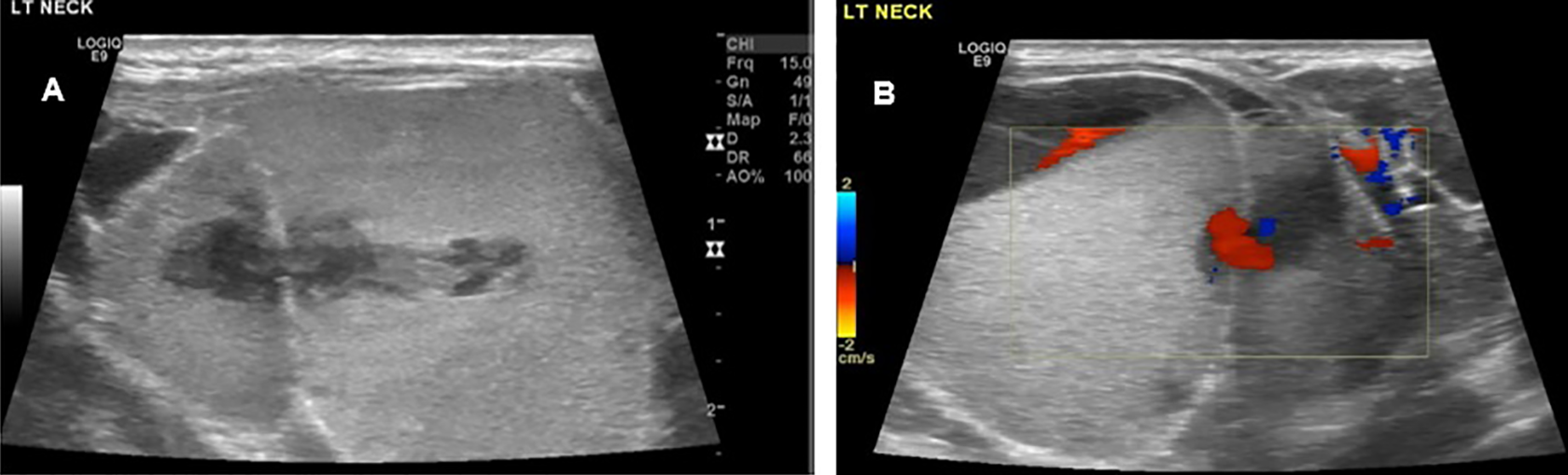
Left side of the neck: (A) gray scale and (B) color Doppler ultrasound, sagittal views, demonstrating a hyperechoic septated cystic mass and occasional vascularity. Findings correspond to lymphangioma complicated by hemorrhage.
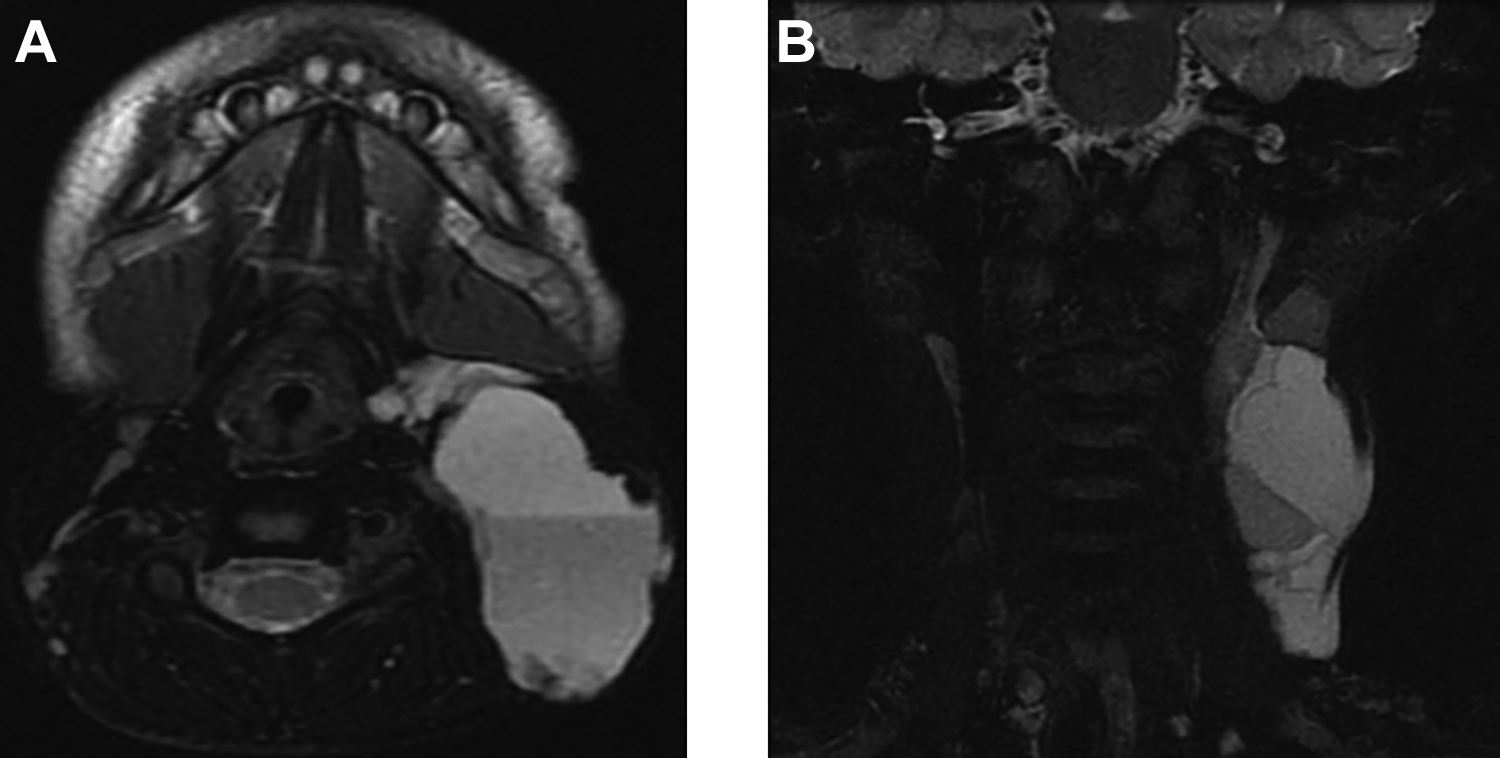
Neck magnetic resonance imaging. T2-weighted images, (A) axial and (B) coronal planes revealing a multilocular, trans-spatial cystic mass with high signal intensity and hematocrit effect on the left side of the neck. Findings correspond to lymphangioma complicated by hemorrhage in a trauma clinical setting.
Discussion
Lymphangiomas are lymphatic malformations with an incidence of approximately 6000 to 16 000 live births, with a 1:1 female to male ratio.1,2 In 75% of the cases, lymphangiomas occur in the neck.1,2 These lesions may be sporadic, subclinical, or asymptomatic, until provoked by a trauma or a viral infection, and can also be part of a syndrome such as Turner, Edwards, or Noonan.1,3,4
Imaging modalities for the diagnosis of neck lymphangiomas include US, CT, and MRI.1,4-7 Ultrasound reveals a multilocular cystic lesion with internal septa of different thickness. Most of the time, cysts are usually anechoic or hyperechoic if there is presence of hemorrhage. 1 At Doppler US, venous or arterial flow may be evident in the septa, giving a possible misleading diagnosis of a vascular malformation or a pseudoaneurysm in a trauma clinical setting.1,4 Computed tomography demonstrates a hypodense, well-circumscribed neck mass. Magnetic resonance imaging shows cystic characteristics with low T1 and high T2 signals, unless there is complication by blood products in which there is evidence of layering and fluid-fluid levels, also known as hematocrit effect. 4
Differential diagnosis for neck lymphangiomas include brachial cleft cyst, teratomas, vascular malformations, among others cystic lesions.1,4
Fine needle aspiration cytology in lymphangiomas has high accuracy and demonstrates occasional red blood cells and mature appearing lymphocytes.8,9 Treatment of lymphangiomas complicated by hemorrhage is complete surgical resection. Conservative management include expectant management, sclerotherapy with bleomycin, aspiration, and radiofrequency ablation.1,2
Footnotes
Acknowledgments
The authors thank Eduardo Gonzalez Toledo, MD, for providing expertise during imaging interpretations and Holly Lorenzen, R.T.(R) VS, for providing technical support during ultrasound study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.