
Abstract

A 25-year-old female was referred to our department with a submental painless mass (Figure 1). Computed tomography showed a well-circumscribed, homogeneous, low-density cystic lesion (25 × 43 × 24 mm) below the geniohyoid muscle (Figure 2). Fine needle aspiration showed a muddy yellow material. Clinical and radiological diagnosis was infrageniohyoid dermoid cyst. As minimally invasive surgery, the patient underwent endoscopically assisted intraoral removal of infrageniohyoid cyst under general anesthesia. After a 2-cm horizontal incision was made in the oral mucosa in the midline of the floor of the mouth through the frenulum (Figure 3A), the genioglossus muscle was exposed in the surgical filed (Figure 3B). A 30°, 4-mm diameter, endoscope with tissue retractor was used for the dissection of deep soft tissues. The tissue retractor mounted to the endoscope was useful to widen the surgical space for dissection and to keep the endoscope tip clean. The genioglossus muscles were separated at the midline and retracted bilaterally to reach the geniohyoid muscles (Figure 3C). Once the median of the geniohyoid muscles was dissected deeply, yellow-white cyst was exposed (Figure 3D). The cyst was dissected carefully from adjacent tissues (Figure 3E) and was removed completely above the mylohyoid muscles (Figure 3F). After the wound was irrigated with sterile saline, careful hemostasis was obtained by bipolar diathermy under endoscopic guidance. The wound was closed as frenectomy after a silicone drain was inserted through the incision site. The drain was removed at first postoperative day, and the patient was discharged 2 days after surgery. Pathology of the specimen showed dermoid cyst. Postoperative course was uneventful, and there was no recurrence 6 years after surgery.

Facial view shows a double chin appearance for submental swelling.
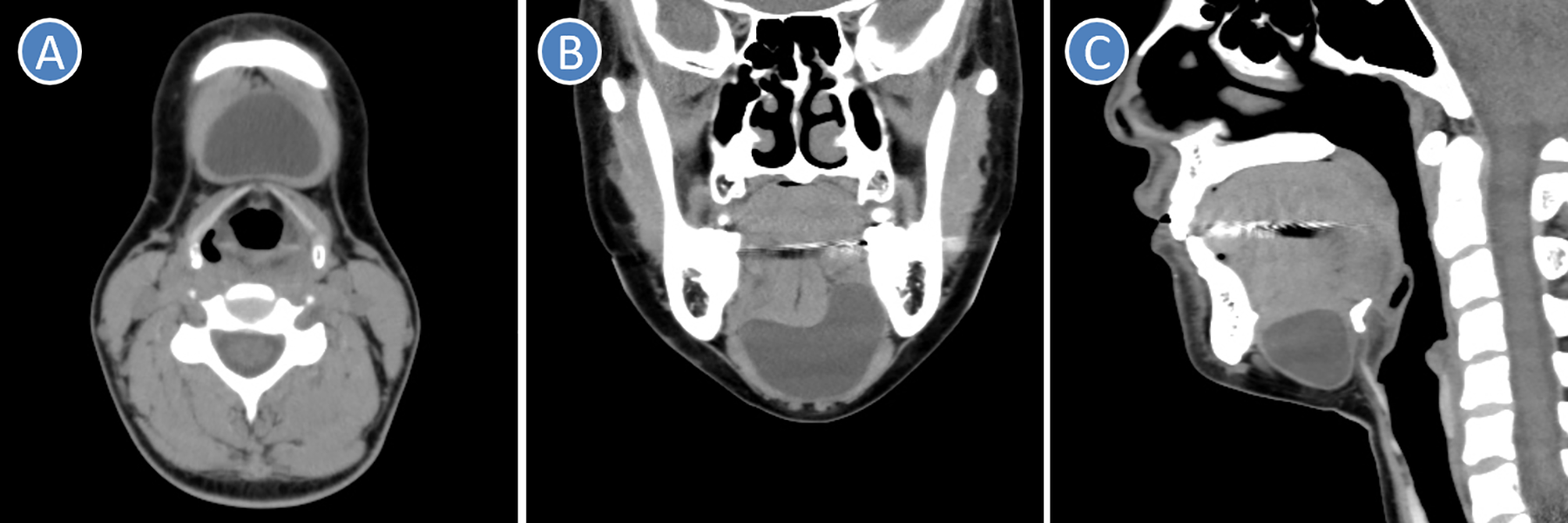
Computed tomography shows a well-circumscribed, homogeneous, low-density cystic lesion (25 × 43 × 24 mm) below the geniohyoid muscle. (A) Axial image, (B) coronal image, (C) sagittal image.
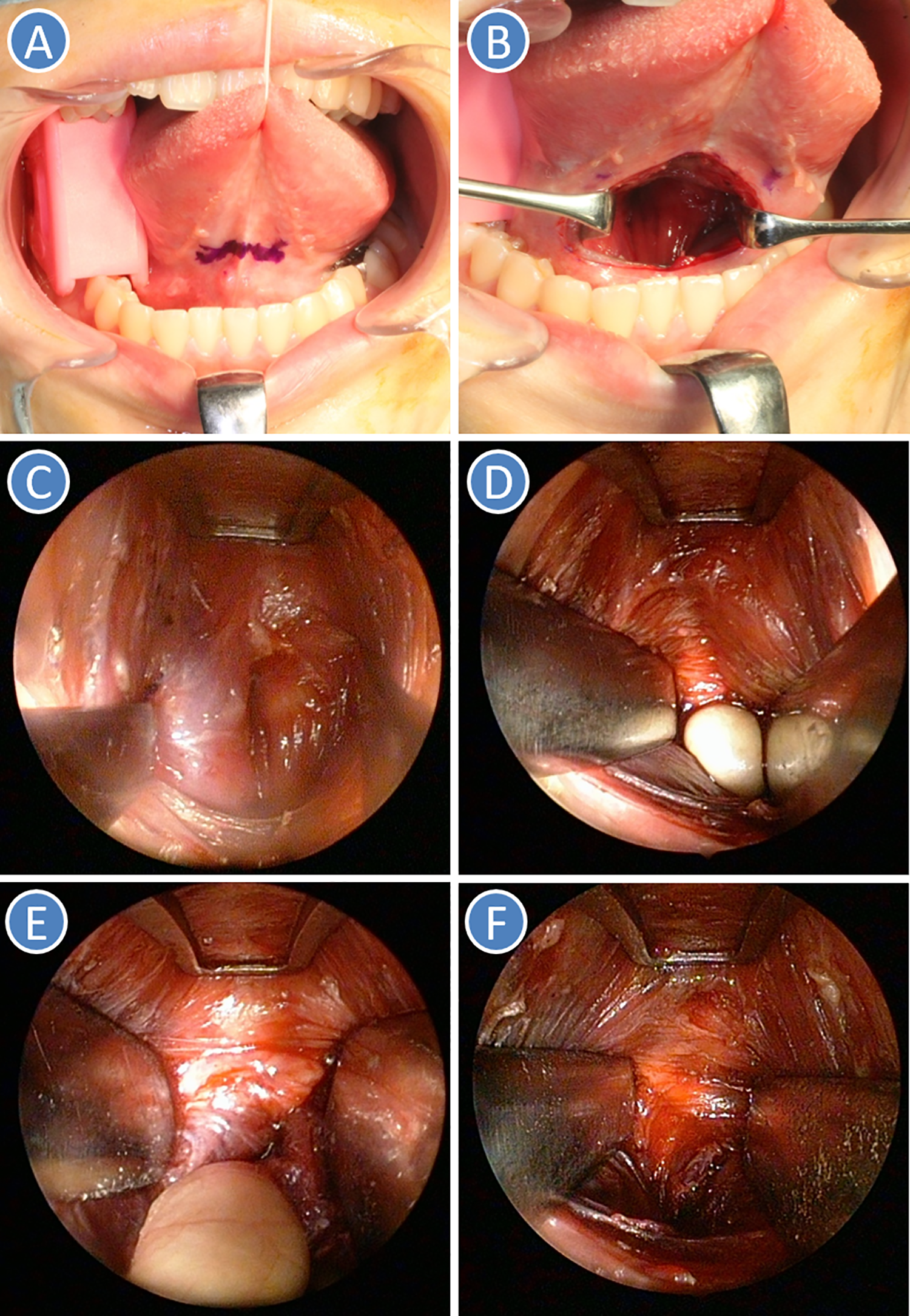
Surgical view. A, Mucosal incision line in the midline in the oral floor through the frenulum. B, The genioglossus muscle was exposed in the surgical filed. C, The genioglossus muscles were separated at the midline and retracted bilaterally to reach the geniohyoid muscles. D, Exposure of dermoid cyst after retraction of bilateral geniohyoid muscles. E, The cyst was dissected carefully from adjacent tissues. F, The cyst was removed completely above the mylohyoid muscles.
Dermoid and epidermoid cysts are slow-growing, benign developmental cysts that arise from ectodermal tissue and can occur anywhere in the body, but most predominantly in the ovary and scrotal regions.1,2 Less than 7% of these cysts involve the head and neck region, with only 1.6% of cases presenting in the oral cavity.1,3 They represent less than 0.01% of all oral cavity cysts. 4 The floor of the mouth is one of the most common sites, however, these cysts can also be found in the tongue, lips, buccal mucosa, and jaw bones.1,3 These cysts manifest in people between 5 and 50 years (mean, 30 years), predominantly in males (male-to-female = 3:1). 5
Dermoid cysts are derived from epithelial rests that are included during midline union of the first and second branchial arches. The vast majority of dermoid cysts of the floor of the mouth are located in the midline (sublingual: 52%, submental: 26%), 16% involve more than 1 of the 3 possible spaces (sublingual, submental, and submandibular spaces), and only 6% are situated exclusively in the submandibular space where they appear to be lateral neck cysts. 1 Although midline dermoid cysts are commonly classified as 2 types (sublingual and submental types) by relationship between the mylohyoid muscle and cyst, Woo et al 6 classified midline dermoid cyst based on relationship between the geniohyoid muscle and cyst as follows: sublingual type (median genioglossal), located between the oral mucosa and geniohyoid muscles; submental type (median geniohyoid), located between the geniohyoid and mylohyoid muscles; and external (median digastric), located between the mylohyoid muscle and the skin. However, submental and external type are inappropriate terms, and some authors had also misunderstood the cyst above the mylohyoid muscle as submental cyst. 7 In contrast, Teszler et al 8 proposed an anatomo-surgical classification of dermoid cyst, and median dermoid cysts were classified as 4 types (suprageniohyoid, infrageniohyoid, submental, and submental transmylohyoid). In present case, dermoid cyst was infrageniohyoid type.
Surgical approach depends on the localization and size of the cysts. Intraoral approach can be performed for sublingual dermoid cysts.2,4,7,9 Extraoral approach with visible scar is commonly preferred,2,4,10 because intraoral removal of infrageniohyoid and submental dermoid cysts is very challenging for limited surgical access and poor visualization. Therefore, endoscopically assisted intraoral approach has been introduced as minimally invasive surgery.2,6 Because endoscope can provide good illumination and visualization in deep and limited surgical field, endoscopically assisted intraoral removal of dermoid cyst is safe and minimally invasive procedure with good esthetic results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.