
Abstract
This report describes the first use of a novel workflow for in-house computer-aided design (CAD) for application in a resource-limited surgical outreach setting. Preoperative computed tomography imaging obtained locally in Haiti was used to produce rapid-prototyped 3-dimensional (3D) mandibular models for 2 patients with large ameloblastomas. Models were used for patient consent, surgical education, and surgical planning. Computer-aided design and 3D models have the potential to significantly aid the process of complex surgery in the outreach setting by aiding in surgical consent and education, in addition to expected surgical applications of improved anatomic reconstruction.
Keywords
Introduction
As the poorest country in the Western Hemisphere, Haiti has severe resource limitations. The strained health care infrastructure combined with low wages (equivalent of ∼$450US/annually) precludes access to medical and surgical care for many. As part of a collaborative surgical outreach program, our group has provided complex head and neck care in conjunction with a team from the University of Haiti. 1 Advanced presentation of odontogenic tumors is common and often prompted by severe deformity, dysfunction, and social ostracization. Tumors frequently are large and disrupt the buccal cortex making anatomic plating for reconstruction of the mandible difficult. To improve outcomes, patient consent, and surgical training, we employed a novel cost-effective rapid-prototyping method for surgical modeling.
The value of using 3-dimensional (3D) printing to plan surgery, specifically in maxillofacial reconstruction, is to reduce operative time and increase both patient and surgeon confidence in the procedure.2-7 The use of prebent plates in mandibular reconstruction using patient-specific 3D modeling techniques has been reported to significantly decrease operative time and improve accuracy of the reconstruction. 8 It was recognized that time savings, while valuable in a high-resourced setting, could be even more valuable in a low-resourced setting, such as Haiti, where operating time and supplies are very limited. A combination of low-cost desktop 3D printers, open-source software, and inexpensive materials has enabled development of in-house 3D printing labs, reducing the cost of each mandible model to approximately $5 to $15 total in materials and machine time. We describe the first reported cases of application of 3D modeling in a resource limited surgical outreach program.
The surgical outreach program has been in operation for 5 years and has had a focus of providing care for Haitian patients and advanced head and neck and reconstructive training for the Haitian surgical team. 3-dimensional models were used as another tool in the educational program to better develop spatial skills necessary for reconstructive surgery.
Case Reports
The 2 cases involved a 21-year-old and 25-year-old female patient (Figure 1C and D) with large ameloblastomas involving the right mandible requiring segmental mandibulectomy with fibula free flap reconstruction. Initially, preoperative computed tomography scans for 2 patients were obtained locally (Port-au-Prince, Haiti) and mailed to our institution. The Digital Imaging and Communications in Medicine data sets were extracted and imported into 3D Slicer (slicer.org) (Figure 1A). Within 3D Slicer, a digital 3D model of the region of interest (ROI) was created by initially using a thresholding tool to segment bone, and then manually correcting the selected ROI to ensure an accurate representation of the anatomy and pathology. This model was exported from 3D Slicer as stereolithography files for digital post-processing in Meshmixer (Autodesk Inc). After validation of the rendering, models were imported into Ultimaker Cura (Ultimaker B.V.) to prepare the file for 3D printing and then printed using white thermoplastic, polylactic acid, on desktop 3D Printers (S5, Ultimaker B.V.). The final 3D printed models were transported to Haiti by the surgical team.
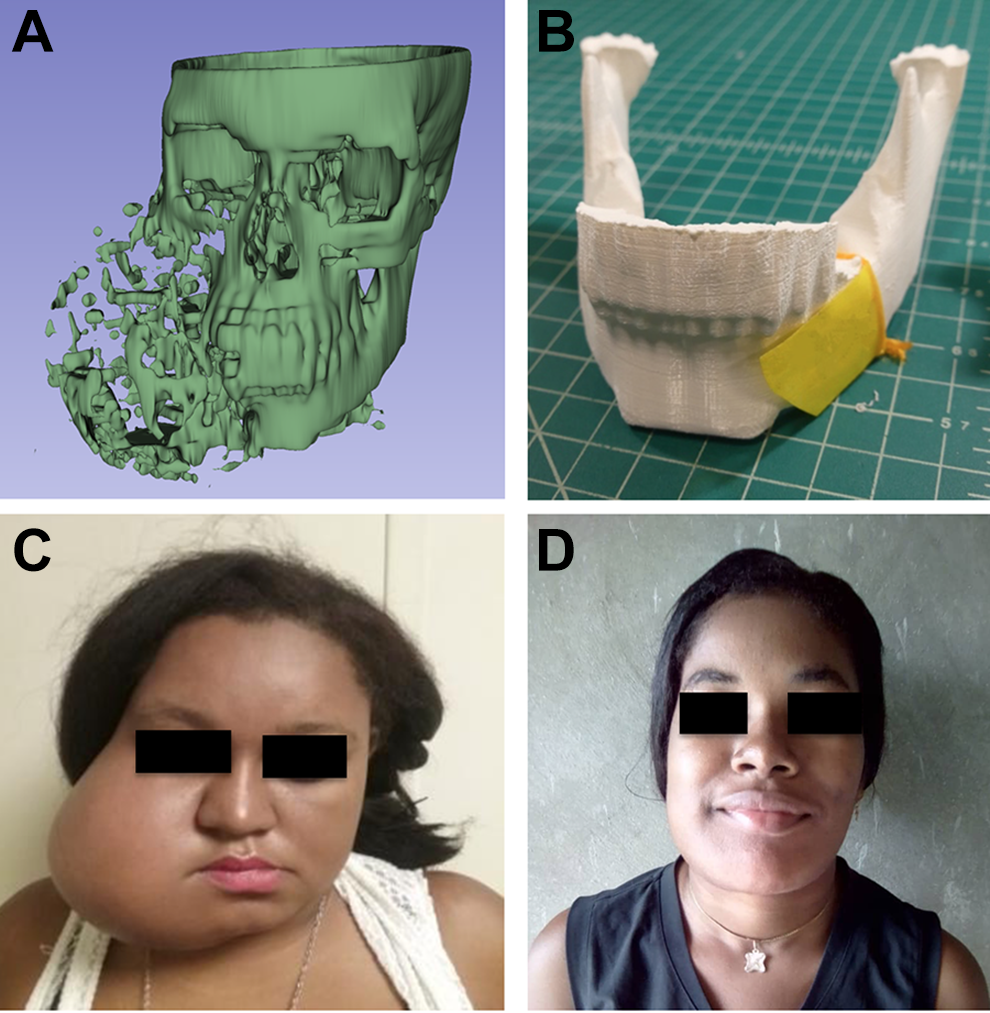
(A) Virtual 3-dimensional (3D) model of a 25-year-old patient with large right-sided lesion recreated using opensource software. (B) Printed 3D model with left-sided hemimandible mirrored to create a template for intraoperative plate bending. (C) Preoperative image of a 25-year-old patient with large right-sided ameloblastoma. (D) Postoperative image of a 25-year-old patient at 1-month follow-up.
Using computer-aided design (CAD) rendering tools in both 3D Slicer and Meshmixer, the 3D rendering for both patients was manipulated, and pathological ROI removed, to allow for the 3D printed models to be used to prebend plates prior to surgery. The ROI for one patient was manually contoured with a rasp to anatomic fit to overcome the problem of significant buccal cortex disruption, and in the second larger tumor, the normal hemimandible was mirrored in Meshmixer prior to 3D printing (Figure 1B) to replace the destroyed tumor side. Completed models aided in the consent process and was reviewed with the patient. In each case, the model was used to obtain an optimized anatomic template for the reconstructive plate prior to completion of osteotomies on the fibula. Plate bending required 7 and 9 minutes, respectively. Upon completion of the ablative portion, the plate was fixated to the residual mandible with minimal adjustments, fibular osteotomies were performed, and the neomandible was created. Total ischemia time for the 2 operations was 115 minutes and 170 minutes. The patients had an uneventful postoperative course, with discharge on day 3, with uneventful postoperative follow-up at 1-week and 1-month with the Haitian head and neck attending.
Discussion
We report the first use of surgical modeling for mandibular microvascular reconstruction (MVR) in the surgical outreach setting which was facilitated by a cost-effective in-house CAD workflow. In a region of low health care and overall literacy, personalized anatomical models offer a novel means of educating patients and aiding in the consent process. 3-dimensional models have been shown to improve patient surgical consent by increasing patient understanding of anatomy and surgery compared to traditional consent processess.6,9 The models were used in conjunction with translators to aid in communication of the plan to patients prior to surgery. The consent process is challenging in this setting due to the need for translation and the use of models helped to produce higher confidence for the surgical team that the patients had an improved understanding of the plan. Although no formal evaluation process was implemented to understand patient satisfaction, the 2 patients anecdotally reported high satisfaction with the use of the model.
The models allowed the surgical team to overcome the challenges of large mandibular tumors: (1) disruption of the buccal cortex preventing anatomic plate templating from the native mandible, and (2) total destruction of mandibular anatomy. These problems were overcome by (1) templating using the 3D-printed model and (2) mirroring the normal hemimandible. Plating for large tumors such as these may often involve some freehand work increasing the likelihood anatomically incorrect fit and can be time consuming.
The models allowed for decreased operative time for plate bending and planning of the fibular osteotomies. The total ischemia time in both cases remained under 3 hours despite the complexities of large multi-segment bony reconstruction, ensuring that the risk of partial loss of flap and other complications were significantly reduced. 10 Potential decreases in deep venous thrombosis rates, hypothermia rates, intravenous fluid use, and anesthetic use due to reduced operative time are additional patient and cost level benefits under consideration in this setting. 3-dimensional modeling has been reported to decrease procedure and ischemia time of mandibular reconstruction with a fibular free flap.3,11,12 The models allowed primarily for improved anatomic fit and decreased overall operating time as the plate bending is typically performed outside of ischemic time. Leong et al in 2006 found a decreased procedure time was associated with decreased incidence of surgical site infection. 10
This study offers preliminary data on the use of a novel workflow for in-house CAD for cost-effective 3D modeling in the surgical outreach setting. These cases suggest that modeling could improve the process of MVR of the mandible, aide patient consent and education, surgical training, and improve anatomic plating adding value for all parties. As such, there are many areas available for investigation during future trips such as bringing a 3D printer onsite to remove the need for transportation of models and patient data, adding patient surveys to gauge understanding and satisfaction with use of the 3D-printed models, and creating workflows and training local teams to incorporate 3D printing into more diverse use cases.
Supplemental Material
Supplemental Material, sj-png-1-ear-10.1177_09544062211015787 - Initial Experience Using 3-Dimensional Printed Models for Head and Neck Reconstruction in Haiti
Supplemental Material, sj-png-1-ear-10.1177_09544062211015787 for Initial Experience Using 3-Dimensional Printed Models for Head and Neck Reconstruction in Haiti by Swar Vimawala, Terry Gao, Jared Goldfarb, Dominick Gadaleta, Bon Ku, Patrick Jean-Gilles, Adam Luginbuhl, Robert Pugliese, Donald Weed and Joseph M. Curry in Ear, Nose & Throat Journal
Supplemental Material
Supplemental Material, sj-png-2-ear-10.1177_09544062211015787 - Initial Experience Using 3-Dimensional Printed Models for Head and Neck Reconstruction in Haiti
Supplemental Material, sj-png-2-ear-10.1177_09544062211015787 for Initial Experience Using 3-Dimensional Printed Models for Head and Neck Reconstruction in Haiti by Swar Vimawala, Terry Gao, Jared Goldfarb, Dominick Gadaleta, Bon Ku, Patrick Jean-Gilles, Adam Luginbuhl, Robert Pugliese, Donald Weed and Joseph M. Curry in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
Meeting: Oral Presentation at 3rd Annual Global Jefferson Day; April 1, 2019; Philadelphia, PA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.