
Abstract

A 62-year-old man presented with left ear fullness, hearing loss, intermittent otorrhea, and vertigo. His examination revealed an intact left tympanic membrane with bulging of the inferior half of the drum (Figure 1). His preoperative audiogram demonstrated a mild to moderate high-frequency sensorineural hearing loss on the left side and a mild high-frequency sensorineural hearing loss on the right side. A temporal bone computed tomography (CT) scan demonstrated a broad-based left petrous apex lesion with bony erosion of the floor of the internal auditory canal, a portion of the carotid canal, and the basal turn of the cochlea, with extension toward the middle ear and hypotympanum (Figure 2A). A magnetic resonance imaging (MRI) demonstrated a complex cyst with communication to the inferior aspect of the internal auditory canal, which was bright on both T1 and T2 images, consistent with a cholesterol granuloma (Figure 2B). He then underwent a left postauricular, infracochlear approach to the petrous apex with drainage of the cholesterol granuloma. He did well in the initial postoperative period but later developed recurrent symptoms including intermittent left otorrhea. His examination again revealed bulging of the inferior half of the left drum. A repeat CT scan showed similar findings as before but also further extension of the lesion into the middle ear cavity and the left inferior external auditory canal (EAC; Figure 2C). He underwent a left postauricular canal wall-up mastoidectomy and infralabyrinthine approach to the petrous apex to drain the lesion. Postoperatively, he had no otorrhea or vertigo but developed left-sided pulsatile tinnitus; however, his symptoms gradually improved and he became asymptomatic. His postoperative examination revealed a recess of the EAC floor where the cholesterol granuloma previously bulged (Figure 3). His postoperative audiogram revealed a mild to moderate high-frequency sensorineural hearing loss on the left side and a mild high-frequency sensorineural hearing loss on the right side. A repeat MRI revealed an overall decrease in the size of his left-sided cholesterol granuloma (Figure 2D).

Left tympanic membrane with a lesion that is bulging posteroinferiorly with extension into the inferior aspect of the external auditory canal.
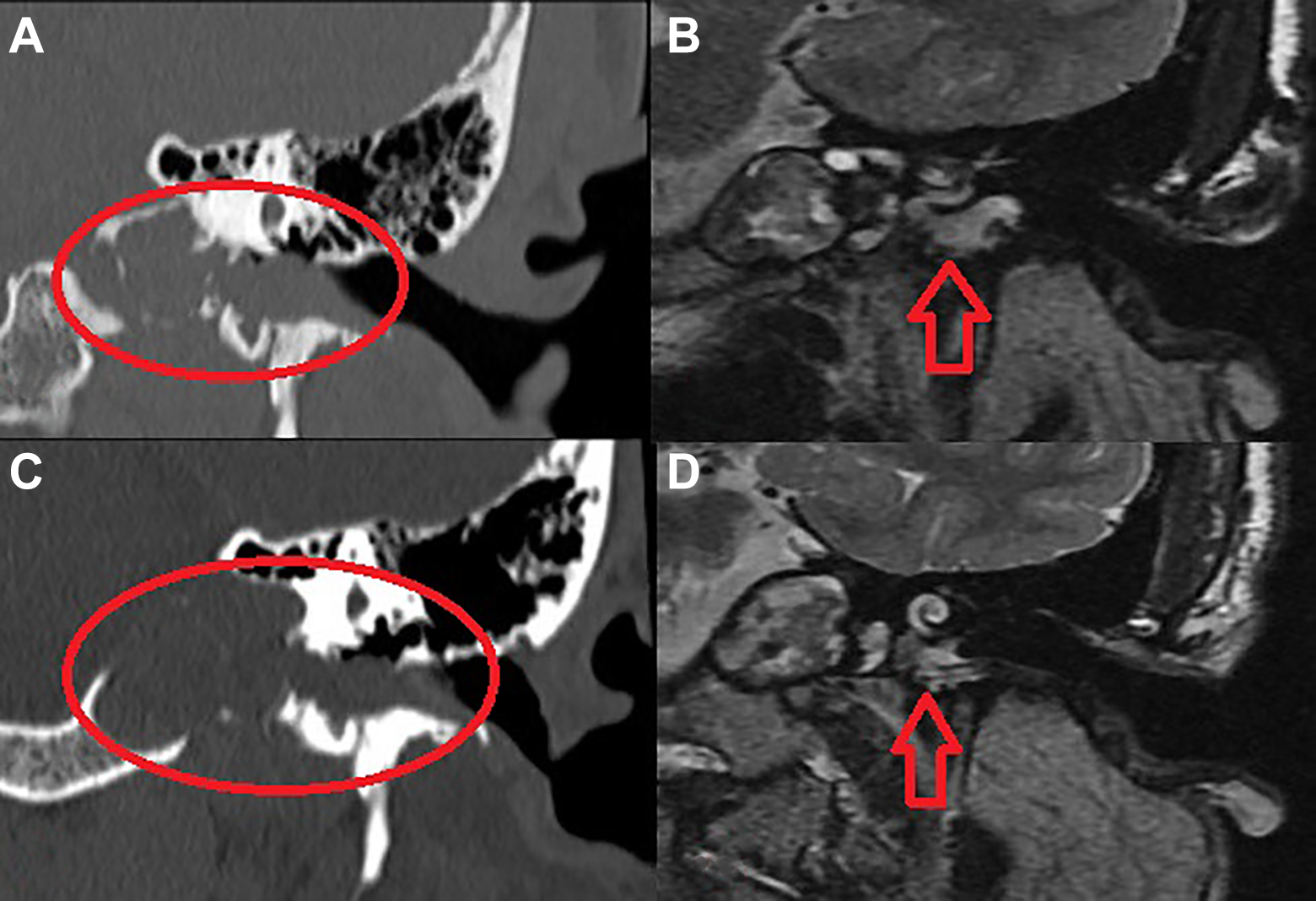
Coronal imaging of the left temporal bone (A) Preoperative computed tomography (CT) scan revealing a left petrous apex lesion. (B) Preoperative magnetic resonance imaging (MRI) revealing a cystic structure bright on T1 and T2. (C) Repeat imaging after first procedure revealed similar findings with erosion into the hypotympanum and inferior aspect of the external auditory canal (D) MRI after second procedure with decrease in size of cholesterol granuloma. Red circles and arrows represent extent of cholesterol granuloma.

Postoperative drainage of the left cholesterol granuloma: posteroinferior aspect of the left tympanic membrane no longer bulging with recession of the bulge previously present along floor of the external auditory canal.
Cholesterol granulomas represent the most common cystic lesion of the petrous apex yet are still rare overall. 1 They are often found in young to middle-aged patients with a history of chronic otitis media, temporal bone surgery, or temporal bone trauma. 2 The pathogenesis is believed to involve a chronic granulomatous inflammatory reaction to hemorrhage and hemoglobin within the pneumatized spaces of the temporal bone. 3 Histology demonstrates cholesterol crystals with a granulomatous inflammatory background. 4 These rare lesions are found infrequently in the middle ear space and are exceedingly rare in the EAC. 2 Here, we provide unique images of a petrous apex cholesterol granuloma manifesting as a bulging lesion within the EAC, both before surgery and after surgical decompression.
Clinical presentation is based on the location of the cholesterol granuloma. With EAC lesions, there have been varying presentations. One case discussed a patient who presented with hearing loss, ear fullness, and obstruction of the EAC by a mass without involvement of the tympanic membrane. 4 Another case had a similar presentation with a patient with hearing loss and a mass occupying the EAC, perforation of the tympanic membrane, with extension into the mastoid with no other symptoms. 2 Yet another patient presented with an asymptomatic, nontender, cystic lesion of the EAC. 5 Other patients may present with a blue and bulging tympanic membrane, tinnitus, vertigo, cerebrospinal fluid leak, and headaches, and possibly facial nerve paralysis depending on the extension and origin of the lesion.1,2 A temporal bone CT scan can reveal a well-circumscribed lesion with adjacent bony erosion. 6 In our case, the bony erosion was extensive and included the carotid canal, the basal turn of the cochlea, and the inferior aspect of the EAC and the IAC. Magnetic resonance imaging can show a hyperintense appearance on T1- and T2-weighted imaging with a hypointense appearance on diffusion-weighted imaging. 6
Management is based on the location and size of the lesion, as well as symptoms. Observation with serial MRI imaging and neurological examinations is possible for asymptomatic petrous apex lesions. 7 If the patient is symptomatic then complete surgical excision or drainage are the treatment modalities of choice whether in the petrous apex, the middle ear space, or the EAC. 1 With involvement of the petrous apex, an infralabyrinthine or infracochlear approach is the surgical approach of choice.1,8 Due to easier access compared to petrous apex cholesterol granulomas, some authors advocate drainage or excision of middle ear and EAC cholesterol granulomas regardless of symptoms, due to risk of eroding crucial structures such as the facial nerve or ossicular chain.1,8 These lesions tend to have a very high recurrence rate of approximately 60%. 9 This is exemplified in our patient who required a repeat surgery involving a mastoidectomy to allow for decompression of the cholesterol granuloma. After the second surgery, he maintained spontaneous decompression and did not experience any further otorrhea. There are 2 primary strategies to prevent recurrence: drainage or surgical resection. 9 A silicone drain placed between the petrous apex and mastoid air cells can allow for aeration and drainage; however, the recurrence rates tend to be high at 22%. 9 Complete surgical resection tends to have lower recurrence rates at 3% and is the more commonly employed treatment modality. 9
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.