
Abstract

Dyskeratosis congenita (DC) is a rare, inherited bone marrow failure syndrome,1-3 and there are 3 inheritance modes: X-linked recessive, autosomal dominant, and autosomal recessive. 4 It is characterized by 3 features: nail dystrophy, reticular skin pigmentation, and oral leukoplakia.1,5,6 Leukoplakia is usually oral, but sometimes conjunctival, urethral, genital, or intestinal.5,7 Oral leukoplakia in patients with DC has a high risk of malignant transformation.4,8 The most frequent solid tumors were head and neck squamous cell carcinoma (SCC) including oral SCC. 3
A 40-year-old male was diagnosed dermatologically as DC for oral leukoplakia, reticular skin pigmentation, and nail dystrophy 19 years ago (Figure 1). He presented to other hospital for enlargement of right buccal mucosa leukoplakia 2 years ago, and the biopsy specimen showed no malignancy. Because he had swelling and ulcer of the right buccal mucosa 2 years later, a biopsy was performed. Because the diagnosis was SCC, he was referred to our department for the treatment of right buccal mucosa cancer. Intraoral examination showed an ulcerative mass (47 × 45 mm) with induration of the right buccal mucosa (Figure 2). Magnetic resonance imaging (MRI) revealed the tumor extended to the right buccal space (Figure 3A and B). Contrast-enhanced computed tomography revealed the right buccal tumor and submandibular lymph node enlargement (Figure 3C and D), and fluorodeoxyglucose (FDG) positron emission tomography/MRI showed high FDG uptake of the right buccal tumor and submandibular lymph node (maximum standardized uptake values = 10.0 and 4.2, respectively; Figure 3E and F). Based on these imaging findings, the diagnosis was buccal mucosa cancer (T4aN1M0, stage IVA). Because the patient refused radical surgery, retrograde superselective intra-arterial chemoradiotherapy was performed as organ preservation therapy. Catheterization from the superficial temporal and occipital arteries was performed, and the catheters were inserted into tumor-feeding arteries such as the maxillary and facial arteries. The dose of docetaxel was 10 mg/m2/wk (total 60 mg/m2) and that of cisplatin was 5 mg/m2/d (total 135 mg/m2). Conventional radiotherapy was performed at 2 Gy/fraction/day, and the total dose was delivered in 54 Gy of scheduled 60 Gy for severe mucositis and dermatitis. Because local recurrence occurred 5 months after chemoradiotherapy, he underwent radical surgery with reconstruction. Although adjuvant chemotherapy was performed, he died for tumor recurrence in the parapharyngeal space 6 months after salvage surgery.

Reticular skin pigmentation (A) and nail dystrophy of hand and foot (B and C).

Intraoral view. The patients had an ulcerative mass with induration of the right buccal mucosa.
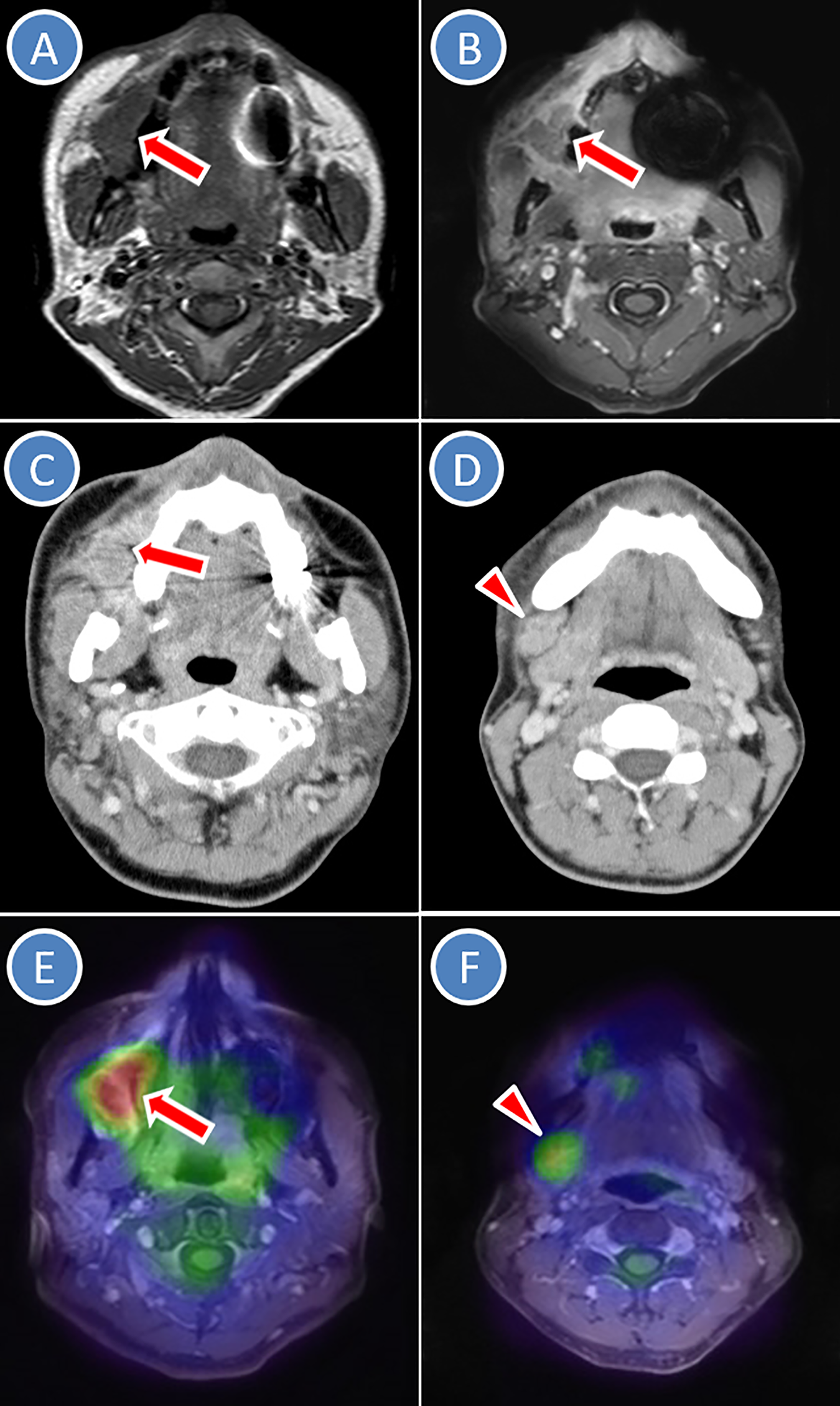
Radiological images: A and B, Magnetic resonance imaging (MRI) revealed the tumor (arrow) extended to the right buccal space on T1-weighted and Gd-enhanced T1-weighted images. Contrast-enhanced computed tomography revealed the right buccal tumor (arrow) and submandibular lymph node enlargement (arrow head). E and F, fluorodeoxyglucose positron emission tomography (FDG-PET)/MRI showed high FDG uptake of the right buccal tumor (arrow) and submandibular lymph node (arrow head).
Patients with DC have potential risks of bone marrow failure, aplastic anemia, myelodysplastic syndrome, leukemia, and other cancers including oral SCC. 6 Dyskeratosis congenita occurs mostly in males and clinically manifests between 5 and 12 years. 8 Nail dystrophy and skin pigmentation appear first by the age of 10 years, and leukoplakia and epiphora develop later. 4 Bone marrow failure and malignant lesions develop in the second and third decades of life. 4 Patients with DC have a 40% to 50% cumulative incidence of risk of malignancy by age 50 years. 8 Prognosis is poor, and the average age of death is 24 to 30 years. 4
Oral leukoplakia occurs in as many as 80% to 90% of patients with DC8,9 and generally manifests between ages 5 and 14 years. 9 In recent systematic review and meta-analysis, the malignant transformation rate of oral leukoplakia was 9.5%, 9 whereas approximately 30% of the leukoplakic areas progress to malignant transformation with the development of SCC in 10 to 50 years.1,2,4-8,10 The most common site of oral SCC is the tongue,1-3,5-7,10 followed by the buccal mucosa. 3 Therefore, frequent monitoring and biopsy of suspicious areas to detect possible oral cancer are necessary. Furthermore, smoking cessation and temperance should be recommended.
In patients with DC, dental management is required for taurodontism and severe periodontal disease including gingival inflammation, bleeding, recession, and bone loss that simulate juvenile periodontitis. 8 Furthermore, multiple permanent teeth with decreased root/crown ratios may suggest a diagnosis of DC. 8
In oral cancer treatment of patients with DC, there are several problems: (1) severe mucositis occurs early for high sensitivity of the mucosa to radiation and it is difficult to continue radiotherapy, (2) pancytopenia makes chemotherapy difficult, and (3) the potential for recurrence and multiple cancers appears to be high. 10 In patients with DC who underwent primary radiotherapy including the present patient, treatment interruption or dropout could occur for hypersensitivity to radiotherapy.7,10 For these problems, surgery is commonly selected as primary treatment.1,2
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.