
Abstract
Objectives:
Otosclerosis is a disease process that usually starts around the oval window, causing fixation of the stapes, resulting in conductive hearing loss. Treatment of the conductive hearing loss caused by otosclerosis consists of either rehabilitation with hearing aids or performing surgery. Given the risks of hearing impairment and vertigo associated with the surgery, there has been a desire to advance the practice to minimize the complications. The so-called “non-contact” or “no touch” techniques with the use of various lasers are in current practice. This review article will cover the surgical aspects, the theory behind laser and the various types used in stapes surgery. It will also review the evidence of laser versus conventional stapes surgery and the comparison of different laser types.
Methods:
A literature search up to December 2019 was performed using Pubmed and a nonsystematic review of appropriate articles was undertaken. Keywords used were stapes, surgery, laser, stapedectomy, and stapedotomy.
Results:
Overall, there is no evidence to say laser fenestration is better than conventional fenestration techniques; however, with the micro drill, there is an increased risk of footplate fracture and sensorineural hearing loss. There is an increased risk of tinnitus with the laser compared to conventional techniques. Studies have favored the CO2 laser over potassium titanyl phosphate (KTP) and erbium-doped yttrium aluminium garnet (Erbium-YAG) lasers for postoperative closure of the air-bone gap; and KTP laser has less thermal, mechanical, and sound effects compared with the thulium and carbon dioxide (CO2) lasers. There is an increased risk if inner ear complications with the thulium laser.
Conclusions:
It can be deduced that theoretically and practically, the thulium laser is less safe compared to the KTP and CO2 lasers. The choice of laser used depends on the surgeon’s preference, as well as availability, cost, side effects profile, as well as ease of use.
Introduction
Otosclerosis is a disease characterized by a process of otospongiosis, resorption of healthy bone, and replacement with abnormal bone tissue. This process usually starts around the oval window, causing fixation of the stapes, resulting in conductive hearing loss.
Treatment of conductive hearing loss caused by otosclerosis consists of either rehabilitation with hearing aids or performing surgery. The surgery itself has evolved from total excision of the stapes (stapedectomy) to further minimal mobilization techniques utilizing various prostheses (stapedotomy). The surgeon has been aided with an advance in technology; from the use of the microscope to performing the surgery either with the assistance of the endoscope or undertaking pure transcanal endoscopic ear surgery. Given the risks of hearing impairment and vertigo associated with the surgery, there has been a desire to advance the practice to minimize the complications. The so-called “non-contact” or “no touch” techniques with the use of various lasers are in current practice.
This review article will cover the surgical aspects, the theory behind laser and the various types used in stapes surgery. It will also review the evidence of laser versus conventional stapes surgery and the comparison of different laser types.
History of Conventional Stapes Surgery and Laser Stapedotomy
Otosclerosis leads to fixation of the stapes footplate in the oval niche and hence a conductive hearing loss. The entire footplate can be removed (stapedectomy), however there is increased risk of perilymphatic leakage resulting in vertigo and a dead ear. The first modern stapedectomy was described by Shea 1 and involved replacing the entire stapes with artificial nylon and covering with a vein graft.
The procedure had been refined by making a fenestration in the stapes footplate (stapedotomy). This can be performed using a micropick or a microburr (using a drill). To gain access to the footplate, the crurae need to be detached. Thereafter, either fat tissue or a vein graft can be used in combination with a prosthesis. They would be placed in the opening and the latter attached to the long process of the incus allowing ossicular chain mobility. Of course, the risks remain as for stapedectomy, which include a floating footplate, vertigo, and sensorineural hearing loss, due to the drill leading to excessive noise and vibration. Numerous authors have described fenestration. However, Fisch 2 found in his series of 392 patients that a small fenestra stapedotomy gave equally good results as a stapedectomy, between 500 and 2000 Hz and better hearing results at 4000 Hz. Given the above, small fenestra techniques became more desirable given the improvement of hearing at higher frequencies but also a reduction in postoperative vertigo was observed. 3
Perkins 4 was the first to describe the use of an Argon laser for stapedotomy in his series of 11 patients. Multiple little perforations in a round fashion were made to allow placement of the prosthesis and is called the rosette technique (Figures 1 and 2). The laser had a fiber-optic cable to a microscope mounted with a micromanipulator; and 50 to 100 µm spot sizes with power settings of 0.4 to 0.7 W at 100 millisesonds, along with a focal length of 160 mm on the microscope were used. Except for some mild dysequilibrium, there were no problems with sensorineural hearing loss or vertigo.
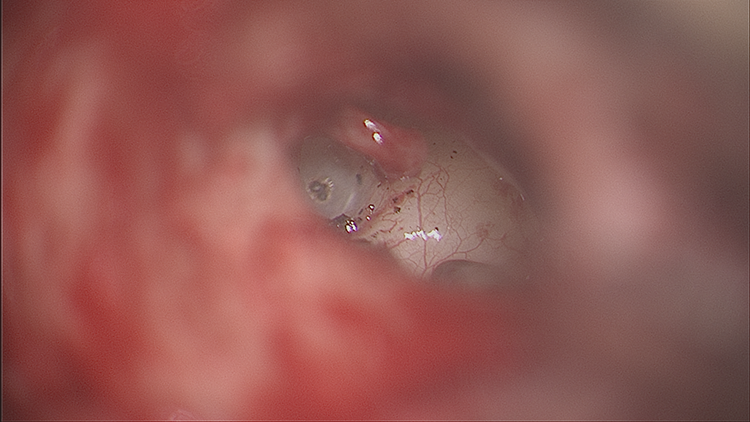
This shows perforations being made with the rosette technique.
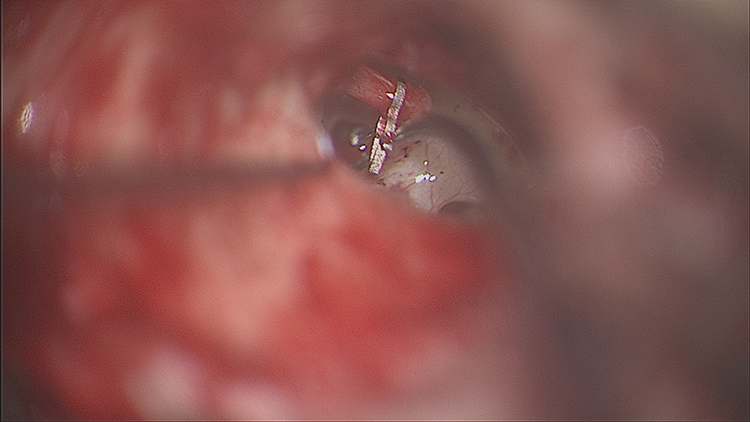
The prosthesis is placed in the footplate and attached to the incus.
The Theory and Practicalities Behind Laser
Laser is an acronym for “light amplification by stimulated emission of radiation.” The basic principles are the photons interact in 3 ways with the atoms: absorption of radiation, spontaneous emissions, and stimulated emission.
They have various properties, which include: Generation of monochromatic light (all the photons have a single wavelength thereby producing a single color). Generation of a collimated beam in which all photons travel in the same parallel direction resulting in a characteristic brightness and forming high concentration of energy when focused onto a small spot. Being coherent (in which the waves or photons travel in steps or in phase with one another in space and time). It can be spatial or temporal and is the most fundamental property of laser.
5
There are 4 tissue effects: Absorption—light energy is absorbed by the tissue and is usually transferred to thermal energy and therefore heating the tissue. Scattering—light spreads through the tissue. Transmission—light exits the tissue leading to loss of laser energy. Reflection—light changes its direction at the surface of the tissue and again leads to loss of laser energy.
6
Basic laser tissue interactions are photothermal, photomechanical, photoablative, and photochemical.
Photothermal interactions require the photons to be absorbed by the tissue they are being applied to, causing a biological effect via a kinetic mechanism. The heat diffusion depends on the thermal properties of the material. The photomechanical effect occurs when the laser strikes the target leading to an acoustic stimulation resulting in a shock wave disrupting the target tissue. Photoablative therapy results in energetic photons of the laser light decomposing the molecules by breaking the chemical bonds. In turn, this can lead to tissue removal without any appearance of thermal damage such as coagulation or vapourization. Photochemical effects of laser don’t lead to a significant rise in temperature and act by excitation of electronic bonds.
There are a variety of laser output patterns. They can be continuous (continuous light emission), pulse (laser energy delivered over a short period of a few nanoseconds with rest periods), Q-switched (obtaining energetic short pulses from a laser), mode locked (pulses of duration of a few picoseconds), and cavity-dumped laser (ultrashort pulses using an optical switch in the laser resonator).
The amount of laser energy that can be delivered to the surface of tissue is measured in Joules per centimetre squared (J/cm2). Parameters that can be altered to adjust the energy being focused here include the pulse length (the duration of exposure) and the spot size (a larger spot will allow dissipation of energy.
Given the above, there are effects that are wanted which include absorption of the laser in the bone leading to stapes footplate ablation. The undesired effects however are vestibule damage due to absorption, resulting in perilymph being affected causing vertigo. Given its connection with the cochlea, this can also lead to hearing loss and tinnitus. 6
The systems used in laser delivery are important and accuracy is key. Argon, diode, KTP, and thulium lasers can be delivered by silica fibers in a handpiece, whereas with the CO2 laser it would be absorbed by silica. Therefore it is delivered using an articulated arm that is linked with a microscope. The arm itself has mirrors that can divert the laser; and with a joystick and micromanipulator, the CO2 laser with the help of an aiming beam can be produced. It is a sophisticated setup, however, the problem that can occur is misalignment due to inappropriate handling of the articulated arm. 6 The ideal laser should therefore be easy to use and handle, have good ablation of bone without penetrating too deeply resulting in unwanted side effects, as well as being cost effective.
Methods
Types of Laser
There are various types of laser in use and the following is a discussion of the benefits and drawbacks of each.
Argon
The argon laser was one of the first lasers to be used in stapes surgery as described above. It has a wavelength of 488 to 514 nm. The low wavelength leads to higher absorption by hemoglobin and is therefore good for hemostasis; and it is also visible therefore no aiming beam is required. However the low absorption in bone means increased penetration of radiation leading to theoretical damage of footplate and inner ear damage. It is used with a handheld fiber-optic micro handpiece.
Carbon dioxide laser (CO2)
It has a wavelength of 9600 to 10600 nm. It has high absorption by bone and therefore reduced depth of penetration and in turn reduced damage to surrounding structures. The disadvantages are the high temperatures involved; and as the beam is invisible it requires a guiding visible laser beam. Previously it had to be attached to a microscope and micromanipulator; but now it is possible to deliver this by a fiber-optic method. In the past, multiple shots were performed to allow the prosthesis to fit; however, currently the CO2 laser can be utilized using the one shot laser technique. 7
Diode
It has a wavelength of 805 to 980 nm and is portable. The wavelengths lie between water and hemoglobin absorption peaks and therefore there is reduced absorption by bone. It uses 2 semiconductor materials that can generate the laser and is delivered by a quartz fiber-optic micro handpiece.
Erbium-doped yttrium aluminium garnet (Erb: YAG)
It has a wavelength of 2940 nm. There is high absorption with water and therefore good absorption in bone and reduced penetration and therefore reduced damage to surrounding tissues (i.e., the inner ear). It does have however poor coagulation capability and can lead to acoustic trauma. It is used with optical fibers.
Potassium titanyl phosphate (KTP)
It has a wavelength of 532 nm and is visible. It has high absorption by hemoglobin because of the low wavelength and has been considered useful in revision stapes surgery. 8 Their retrospective review of 26 patients over 18 years showed no complications of sensorineural hearing loss or deafness. Like the argon laser, low absorption in bone means increased penetration of radiation leading to theoretical damage of the footplate and inner ear damage. The KTP laser can be used with a handheld fiber-optic micro handpiece (Figure 3).
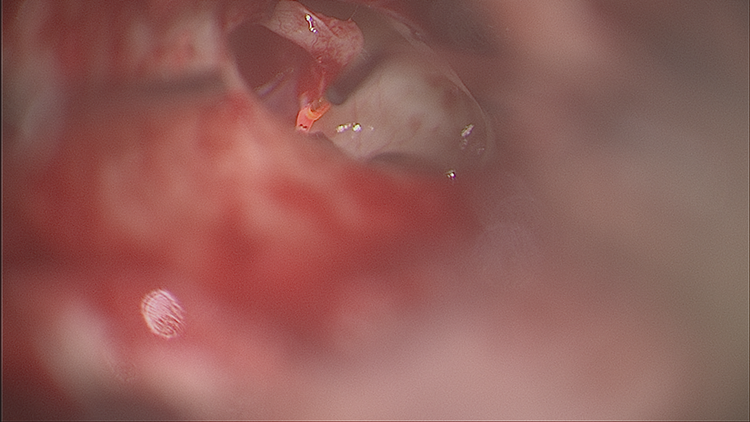
This shows the handheld potassium titanyl phosphate (KTP) laser being applied to the stapedius tendon.
Thulium
It has a wavelength of 2013 nm. It has increased absorption by water and therefore good for hemostasis and also useful for its preciseness for tissue resection. However, in studies it has been shown the temperature is high and it can lead to acoustic shock. It is utilized using a fiber-optic micro handpiece.
Discussion
Laser Versus Conventional Stapes Surgery
Wegner et al
9
conducted a systematic review and showed there are many studies on the effects of laser fenestration versus conventional fenestration. Various factors needed to be considered prior to interpreting the findings. Different lasers and pistons types and sizes were used and the choice of pure tone audiometry frequencies and the follow-up duration of patients varied. There is a risk of bias in these studies due to lack of standardization treatment, test procedures, randomization, and treatment allocation and blinding of observations. The majority of studies had small sample sizes and large sizes are required to make reliable statements about sensorineural hearing loss. There was a lack of systematic evaluation of adverse events.
In the laser group, tinnitus seemed to occur more frequently postsurgery compared to the nonsurgery group. There was however no evidence that either laser fenestration or conventional fenestration techniques are superior to the other technique with regard to hearing outcome or immediate postoperative vertigo. There does, however, seem to be an increased risk of footplate fracture and sensorineural hearing loss following the use of microinstruments or micro drill.
Comparison of Different Laser Types
Kamalski et al 10 conducted a systematic review to evaluate the hearing outcome of stapes surgery with different types of lasers. They included 2 studies that showed a high directness of evidence. There was a difference in postoperative air-bone gap closure in favor of CO2 laser over the KTP or Erbium-YAG laser. Sensorineural hearing loss did not occur in these groups. The risk difference of 28.1% (95% confidence interval, 22.8-33.4) between CO2 and Erbium-YAG favored the CO2 laser.
The clinical interpretation and practical relevance however is yet to be determined. The problems with the studies are that they show bias, lack of randomization, treatment allocation, blinding of observations, and they have poorly standardized treatments. There was also a different approach to laser settings, techniques employed, as well as calculation of the air-bone gap. Some studies showed follow-up of 3 months, whereas the committee of hearing and equilibrium suggest follow-up of 1 year is desirable and gives a more realistic representation.
The same group undertook experimental studies using an inner ear model to compare the thermal and mechanical effects as well as sound production of the CO2, thulium, and KTP lasers. Utilising high speed Schlieren and thermal imaging, they found increased thermal effects beneath the stapes footplate with the thulium and CO2 lasers, compared to the KTP laser. These 3 lasers generated less noise compared to the microburr; however, in their inner ear model, they found the thulium laser produced large bubbles within the vestibule. The KTP laser however produced little mechanical effect and the CO2 laser produced small bubbles within the vestibule. From these studies it can therefore be assumed that from the theoretical evidence, KTP laser has lesser thermal, mechanical, and sound production effects compared to thulium and CO2 laser.
A prospective nonrandomized control study at the Jean Causse Ear Clinic, Beziers, 11 compared the use of the thulium and CO2 lasers. At 3 months, the air-bone gap closure to within 10 dB with the CO2 laser was 96.8% and 90% with the thulium laser. However, there was higher risk of inner ear complications with thulium as they found 4.4% encountered sensorineural hearing loss and 3.1% had tinnitus.
Summary
From the information above, it can be deduced that theoretically and practically, the thulium laser is less safe compared to the KTP and CO2 lasers for example. The choice of laser used depends on the surgeon’s preference, as well as availability, cost, side effects profile, as well as ease of use (e.g. using a handheld fiber compared to the mechanism of delivery with the CO2 laser). Studies do point in the direction of laser being favorable compared to use of the micro drill and the increased risk of footplate fracture and sensorineural hearing loss.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.