
Abstract
Objectives:
Transoral CO2 laser therapy represents the treatment of choice for early-stage laryngeal tumors. The anterior commissure involvement (ACI) is related to a worse local control and a lower rates of organ preservation. The objective of this study is to analyze the differences in survival, local control, and organ preservation in T1b glottic patients according to the presence of ACI.
Methods:
Observational prospective study in pT1b treated with transoral CO2 laser between 2009 and 2014.
Results:
Forty patients (37 male and 3 female) with a mean age of 66.43 ± 8.16 years were recruited. Anterior commissure involvement was present in 70% of the patients. The 5-year specific cause survival was 91.66%, with 32.50% of local recurrences. Laryngeal preservation was 80%, being lower in the group with local recurrence (P < .000). The involvement of the anterior commissure does not influence the organ preservation (P = .548), the appearance of local recurrences (P = .391), or the survival (P = .33).
Conclusions:
Transoral CO2 laser therapy is an effective and reproducible treatment for early-stage laryngeal tumors. The results obtained are similar to previous studies, although they present discrepancies in relation to the role of the ACI. Prospective randomized trials are required focusing also on the patients’ quality of life and functional outcome in order to clarify the role of the ACI and the need to implement changes in its evaluation, staging, and evolution.
Introduction
Laryngeal squamous cell carcinoma (SCC) is the most common neoplasm in the head and neck area, and the glottic localization represents 65% of cases. 1 In recent years, this type of tumors has shown growth in the number of cases and mortality, which is why his treatment continues to generate debate. 1,2
According to the seventh and eighth edition of the TNM-staging system, T1b is defined as cancer in which both vocal cords are involved, 3,4 and also involves the anterior commissure (AC). Transoral CO2 laser therapy (CO2TOLMS), 5 open partial surgery, and radiotherapy represent the treatment of choice for this type of early-stage tumors (T1-T2). 6 -8 Transoral CO2 laser therapy approach allows complex resections, preserving disease-free areas, reducing the need for a tracheostomy and nasogastric tube, as well as obtaining local control of the disease at 5 years between 70% and 100%. 6,9,10
The AC is considered a laryngeal subsite, but it is not taken into account in the current T-staging system. 3,4 This subsite rarely corresponds to the origin of glottic tumors (1% laryngeal tumors), but 20% of glottic tumors show anterior commissure involvement (ACI). 11,12 Its presence and role have been a subject of debate in recent years, and there is controversy regarding the treatment of early glottic cancer with ACI and it is related to a worse local control and a lower rates of organ preservation. 9,13 The objective of this study is to analyze the differences in survival, local control, and organ preservation in T1b glottic SCC patients treated with CO2TOLMS according to the presence of ACI.
Methods
Study Design and Data Collection
A descriptive and analytical observational prospective study in adult patients diagnosed with primary early glottic carcinoma (pT1bN0M0), who were treated exclusively with CO2TOLMS in an Otorhinolaryngology–Head and Neck Surgery Department of a tertiary university hospital with a minimum follow-up time of 5 years between 2009 and 2014. The management and treatment of all patients were discussed in the Hospital’s Multidisciplinary Head and Neck Oncology Committee. This research involved human participants and was approved by the Hospital’s Ethics Committee. Informed consent was obtained from all individual participants included in the study.
Inclusion criteria were to have a confirmed diagnosis, with anatomopathological and computed tomography scan radiological study, 14 of primary pT1bN0M0 glottic carcinoma based on the Seventh Edition of the American Joint Committee on Cancer TNM classification system. 4 Patients were grouped according to the existence of ACI or not. Exclusion criteria were to have synchronous malignancies/distant disease, noncurative treatment intention, need for conversion to open surgery in the same act, noncandidate patients for transoral resection, refused/incomplete treatment, and lack of complete follow-up data (at least 3 months after tumor resection). Exclusion criteria were not applied according to the histological type of the tumor or patient age.
Sociodemographic variables, local control rate (LCR), disease-free survival, laryngeal preservation rate (LPR), salvage surgery, type of laser resection according to the European Laryngological Society, 15 and complications, were collected. The standard follow-up protocol consists of a clinical examination with endoscopic laryngoscopy on a regular basis (every 4-6 weeks in the first, every 2-3 months in the second and third, and every 3-6 months in the fourth and fifth year, respectively).
Surgical Technique
All procedures were performed with the patient under general anesthesia. Suspension laryngoscopy was performed, and the lesion was examined under microscopy (OPMI Vario S88; Zeiss). Cordectomy type Va or III, according to the European Laryngological Society classification, 15 was performed using CO2 laser with an AcuSpot 712 Micromanipulator (Lumenis AcuPulse 30/40W; Adisat), considering an adequate safety margin when it was at least 2 mm from the tumor. When required for adequate glottic exposure, a partial vestibulectomy or Burp maneuver was performed. The surgical specimen was fixed to a soft board, with the margins marked with ink and sent for definitive analysis by an experienced surgical pathologist. No frozen sections were performed.
Statistical Analysis
Statistical analysis was performed with SPSS version 24.0 for Windows (IBM). Statistical tests were 2 tailed with a 95% confidence interval. Normality was evaluated by the Kolmogorov-Smirnov test and variances using the Levene test. Quantitative variables were expressed as mean ± standard deviation and median. The comparison of means between groups was performed using the Student t, Mann-Whitney, analysis of variance, or Kruskal-Wallis test as appropriate. Qualitative variables were expressed as frequency and percentage. The differences between groups were evaluated by the χ2 test, Fisher exact test, or its variants as appropriate. Kaplan-Meier method and further analyzed with the log-rank test for univariate analysis. Patients with a loss to follow-up were censored.
Results
A total of 40 patients who met the inclusion criteria were recruited, 37 male (92.50%) and 3 (7.5%) female. The mean age was 66.43 ± 8.16 years (range: 50-84 years). Anterior commissure involvement was present in 70% (n = 28) of the patients and all were treated with Va cordectomy. The 30% without ACI was treated with type III cordectomy. The pathological result of all resections was SCC.
Follow-Up
The mean time of hospitalization was 1.40 ± 0.84 days, and no postoperative complications were reported. No patient underwent cervical neck dissection or tracheostomy, nor did they require nasogastric tube feeding.
The LCR was of 67.5%, with 13 (32.50%) patients in whom a local recurrence was found. The 61.50% (n = 8) of them were treated with radical surgery (total laryngectomy), 30.75% (n = 4) with CO2TOLMS, and 7.75% (n = 1) with partial open surgery (cricohyoidoepiglottopexy). Therefore, the LPR was 80% (n = 32). Analyzing the group with local recurrence, the LPR was 38.5% (n = 5), there are statistically significant differences compared to the group without local recurrence (P < .000). The mean follow-up time until the clinical diagnosis of local recurrence was 21.26 ± 6.55 months, with 53.55% of these occurring in the first 24 months of follow-up after CO2TOLMS.
The role of ACI in local recurrences and organ preservation was evaluated (Table 1). First, it was found that 77% (n = 10) with local recurrence had ACI compared to 23% without ACI. Comparing these results with the group without evidence of local recurrence, which had 66.7% (n = 18) of ACI, there were no differences (P = .391). Second, no differences were found in organ preservation according to the ACI (P = .548).
Role of the Anterior Commissure Involvement in Local Recurrence and Laryngeal Preservation.
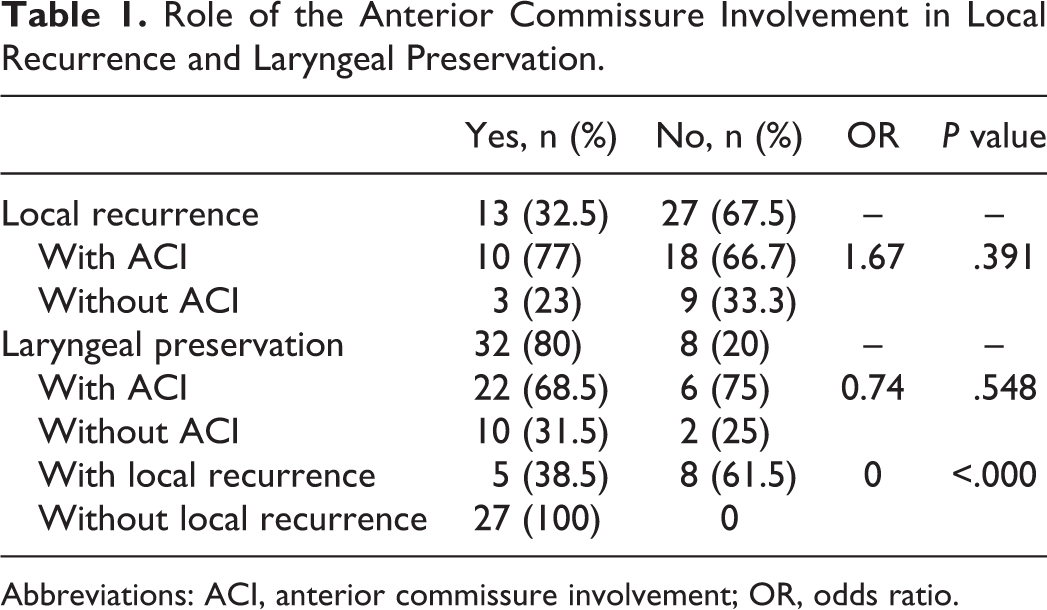
Abbreviations: ACI, anterior commissure involvement; OR, odds ratio.
Survival
The overall survival at 3 and 5 years was 83.7% and 71.9% (Figure 1), respectively, and the specific cause survival was 94.55% and 91.66% at 3 and 5 years, respectively. Statistically significant differences were obtained in relation to specific survival in the group with local recurrences compared to the one that did not present recurrence (P < .000; Figure 2). Regarding the ACI, no statistically significant differences were found in relation to the specific cause survival (P = .33).
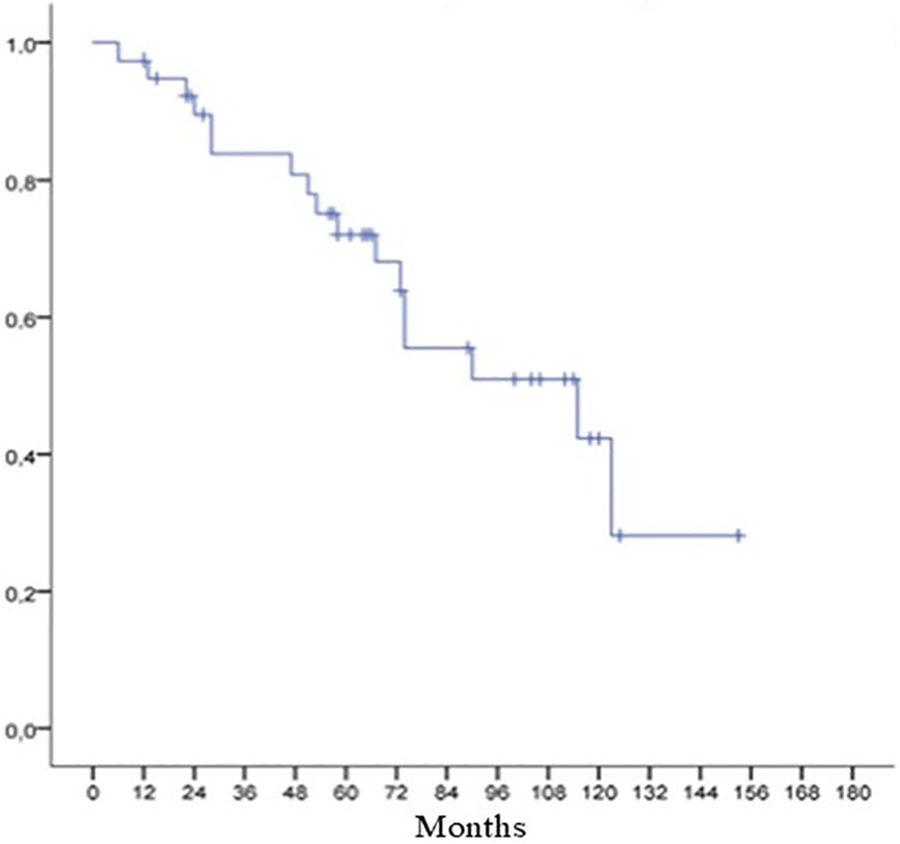
Overall survival at 3 and 5 years.
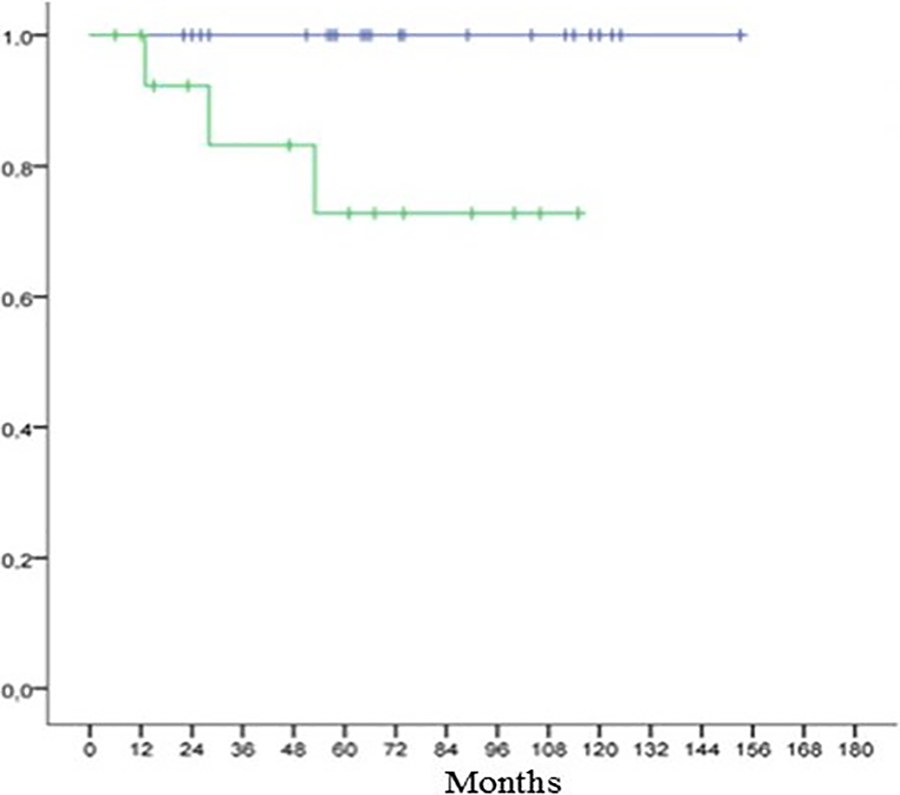
Specific cause survival depending on the presence (green line) or not (blue line) of local recurrence.
Discussion
Laryngeal cancer is the most frequent cancer of the head and neck in both Europe and the United States, with 65% involvement of the glottic area. 1,9 These tumors are generally diagnosed early, which can be treated using minimally invasive therapies like CO2TOLMS, obtaining long-term organ preservation and with good functional results. 6,10,16 In the previous literature, local control has been reported in early stages between 70% and 100%. 9 -11,16 -18 These data seem to be explained by the variability in the sample proportions included according to the TNM-staging system. 9
The term early glottic cancer encompasses T1a, T1b, and T2 stages with different characteristics and that seem to have a different evolution. For this reason, research focused on each stage has been carried out in recent years. 9,19 Specifically, T1b and ACI are the objects of anatomic, diagnostic, and therapeutic controversies in laryngeal oncology. 20 This study represents one of the largest cohorts with T1b cancer involving the AC to date.
The eighth edition of the TNM staging system introduced major changes for some cancers. However, the staging of laryngeal tumors has not undergone any change yet. 3,4 Among the small number of reports, including more than 30 patients with ACI treated by endoscopic laser cordectomy, 9 most have described poorer oncological outcomes for these tumors compared to those sparing the AC. 9,16,21 Likewise, the few studies focused specifically in T1b patients seem to present significantly lower results in relation to LCR and survival compared to previous studies that analyzed the set of early glottic cancer. 13,18 Despite this, the conclusions are not unanimous and the role of the ACI continues to be controversial. 9,22 To date, there are no prospective reports in this regard, so the objective of this study was to analyze the differences in survival, local control, and organ preservation in T1b glottic SCC patients treated with CO2TOLMS according to the presence of ACI.
The findings in relation to ACI in our population are similar to previous studies in which an affectation of 69% was found. 17 The overall and specific survival are also similar to the data described in the previous literature, with values greater than 80% at 3 and 5 years, and without differences in relation to the ACI. 7,16,17,19 While the early-stage glottic carcinoma without AC infiltration treated by CO2TOLMS shows excellent oncologic and functional outcomes, with recurrence rates similar to our work and typically range from 15% to 30%, 17,19 the carcinoma with AC infiltration is often associated with a worse clinical course. 11,16,17 This might be due to a higher rate of local recurrence compared to the carcinomas that are solely placed on the vocal chords. In fact, the influence of local recurrence on the survival found in our cohort is remarkable, being significantly less in the group of these patients. Despite this, no differences were found in the local recurrence rate in relation to the ACI.
In relation to organ preservation, our data are similar to previous literature where rates from 80% to 100% for early-stage glottic tumors have been reported, although it can be improved. 17,23 This fact has been related to various factors such as the inclusion of T1a, T1b, and T2 in the statistical analysis or the ability of T1b to progress into circumscribed T4a tumors due to thyroid cartilage involvement in a short period of time (Figure 3), which represents a contraindication for CO2TOLMS. Hence, some authors even claimed a modified tumor staging classification addressing ACI. 24 The Broyles’s ligament is a weak structure of the AC resulting in peculiar progression pathways of cartilage invasion due to local dehiscence of perichondrium at its insertion point. A CO2TOLMS in T1b glottic SCC demands conditions and superior surgical and anatomical skills from an oncological safety point of view, being necessary to contemplate other treatment modalities such as open partial surgeries or radiotherapy in some lesions with ACI and poor laryngeal exposure. 7,8,11,18,25 These treatment modalities present equivalent oncological results, being in the morbidity and functional results where the differences reside. In this sense, advances in endoscopic surgery, 26 implementing the flexible diode laser, 27 or through transoral robotic surgery 28 have been proposed in order to decrease morbidity and improve tumor exposure.
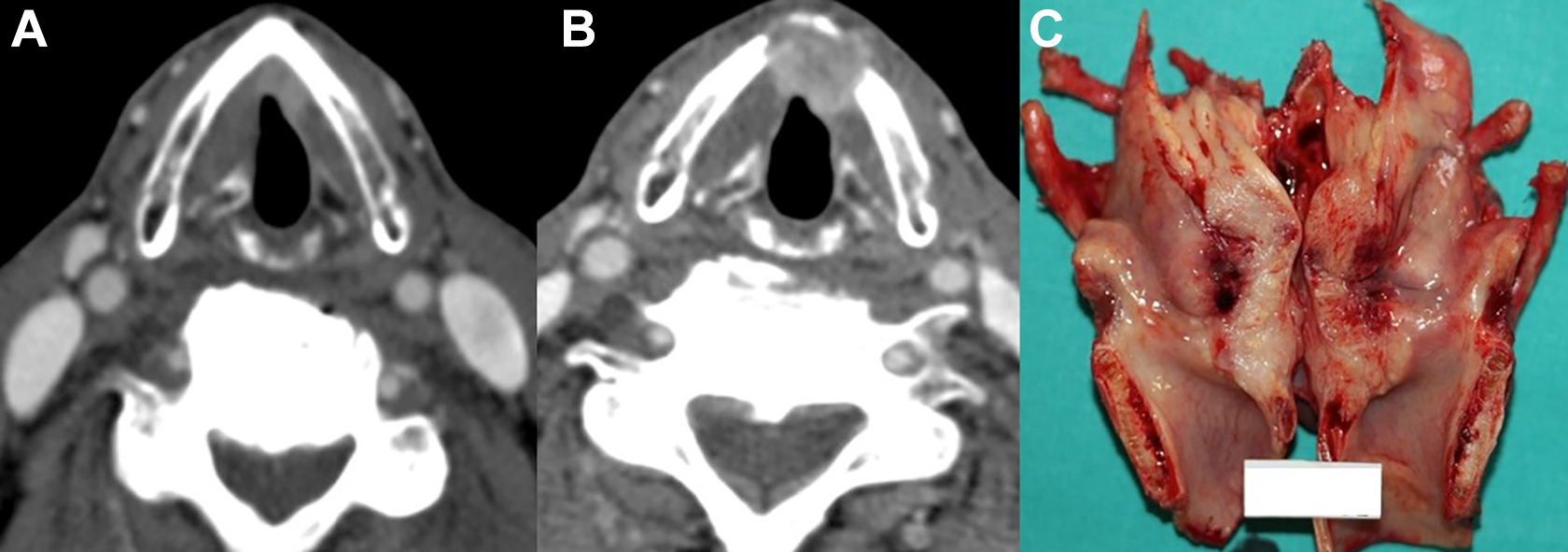
A, Computed tomography scan with T1b glottic tumor with involvement of the anterior commissure. B, T4a recurrence 1 year later, with thyroid cartilage involvement. C, Total laryngectomy due to this recurrence where transglottic extension can be seen.
We must reflect on surveillance and the need for early regulated radiological control in the first postoperative months in order to improve the organ preservation rate. 9,14,19 Likewise, Piazza et al emphasized the need for more detailed staging of early glottic cancer into 6 subcategories to better cope with the wide spectrum of distinct local tumor spread. For this purpose, they classified the range from tumors infiltrating 1 vocal cord to those with horizontal spread to the vocal muscle/paraglottic space, or those with a vertical trans-AC extension with an invasion of the anterior pre-epiglottic/paraglottic space. 24
Conclusion
In conclusion, we present the first prospective data described regarding a homogeneous group of exclusively CO2TOLMS-treated T1b glottic carcinoma patients in which the role of the ACI has been evaluated. According to our results, this is an effective and reproducible treatment for this type of lesions, with similar results to previous studies and comparable with other therapeutic modalities. 8,9,11,21,22 Despite this, prospective randomized trials are required focusing also on the patients’ quality of life and functional outcome in order to clarify the role of the ACI and the need to implement changes in its evaluation, staging, and evolution.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.