
Abstract
A 32-year-old gentleman presented with a 1-year history of multiple atraumatic fractures involving the tibia, fibula, calcaneum, lumbar spine, sacrum, and ribs. On evaluation, he was found to have hypophosphatemia and phosphaturia with normocalcemia and mildly elevated alkaline phosphatase. A low ratio of maximum rate of renal tubular reabsorption of phosphate to glomerular filtration rate (TMP-GFR: 1.9 mg/100 mL) confirmed renal phosphate wasting. His fibroblast growth factor (FGF 23) was elevated, while his vitamin D and parathyroid hormone levels were normal. Normal urine pH and chloride levels ruled out renal tubular acidosis. Genetic causes of phosphopenic osteomalacia were ruled out by detailed family history. Suspicion of a tumor-induced osteomalacia (TIO) warranted evaluation for any oncogenic cause. General examination did not reveal any swellings in the body. A Gallium-68 DOTA-octreotate somatostatin receptor positron emission tomography/computed tomography imaging (Ga-68 DOTATATE PET/CT) showed uptake at the posterior end of the left nasal cavity with no other areas of uptake (Figure 1). This was confirmed by nasal endoscopy (Figure 2) and on contrast CT scan (Figure 1). Complete endoscopic excision of the vascular mass under hypotensive anesthesia was done. Histopathology examination showed a tumor of hemangiopericytomatous pattern, composed of sheets of spindle-shaped cells. Immunohistochemistry was negative for SMA and CD34, thereby suggestive of a phosphaturic mesenchymal tumor (PMT) with a benign angiomatous pattern. Postoperatively, his biochemical parameters completely normalized in 3 months and he continues to be asymptomatic 3 years later.
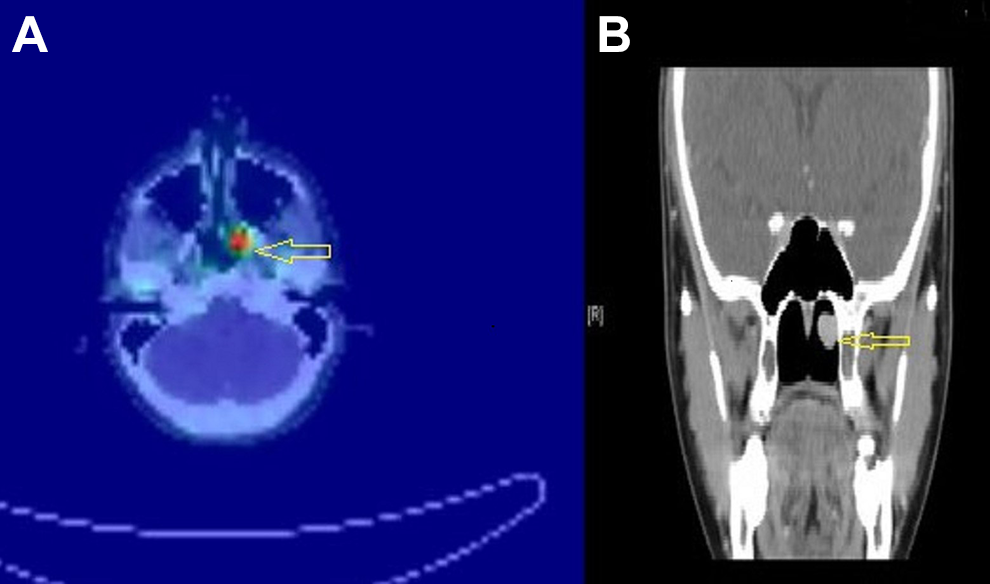
(A) Gallium-68 DOTA-octreotate somatostatin receptor positron emission tomography/computed tomography imaging (Ga-68 DOTATATE PET/CT) axial image on the left showing uptake in the left posterior nasal cavity (yellow arrow) and (B) on the right coronal image on the CT showing an enhancing mass (yellow arrow).
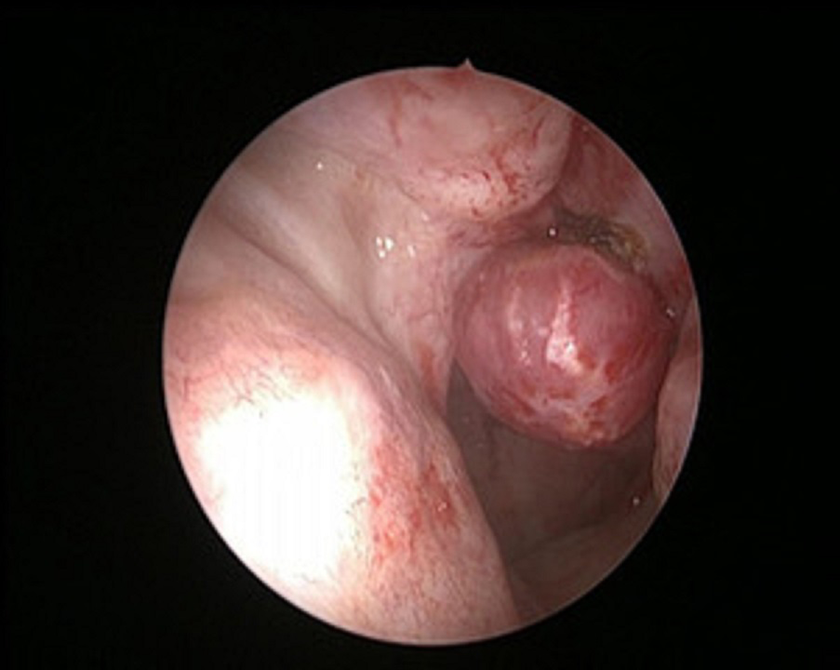
Rigid nasal endoscopy image with black arrow showing a vascular mass in the left nasal cavity.
Tumor-induced osteomalacia is a rare paraneoplastic syndrome, most commonly caused by PMT. 1 It is characterized by hypophosphatemia with renal phosphate wasting and osteomalacia leading to multiple atraumatic fractures. This tumor predominantly affects the appendicular skeleton with predilection for head and neck region seen in less than 5% of these patients, of these more than half are in the sinonasal region. So far around only 30 cases of sinonasal involvement have been reported.2-4
Symptoms include nonspecific weakness, bone pain, and multiple fractures. These are often misdiagnosed to be musculoskeletal or rheumatological in origin. The suspicion is raised when laboratory tests reveal hypophosphatemia, normal or low levels of 1,25-dihydroxyvitamin D, elevated levels of alkaline phosphatase, and normal circulating levels of calcium and PTH.
The initial step would be to determine if it is renal or nonrenal in etiology. A low TMP-GFR with hypophosphatemia as in our patient indicates renal phosphate wasting. Renal causes can be FGF 23 mediated or non-FGF 23 mediated. FGF23-dependant disorders include genetic causes which can be ruled out by detailed family history aided with genetic testing if needed and TIO.5,6 A suspicion of TIO calls for a thorough clinical examination for any new swelling. The imaging protocol which gives the most likely localization includes functional imaging such as octreotide scanning, 18F-FDG (fluorodeoxyglucose) PET/CT, and Gallium and 99mTc bone scintigraphy followed by anatomical imaging such as ultrasound, CT, and magnetic resonance imaging. 7 More recently, Ga-68 DOTATATE PET/CT has been found to be very sensitive. 8
In case of a sinonasal PMT, the otolaryngologist is more likely to find a mass concealed in the ethmoid or maxillary sinus. 2 Even if the lesion is well identified on nasal endoscopy or paranasal imaging, a functional scan such as FDG PET scan is essential to rule out the presence of other tumors. Alternatively, an otolaryngologist may be in a situation where a nasal mass was excised and biopsy revealed PMT. In such case, biochemical parameters must be checked, scintigraphy scan done to rule out other lesions, and patient should be kept on strict follow-up. Most sinonasal PMT can be managed by an endoscopic approach, very rarely the large ones may need combined craniofacial or oral approaches.2-4 These lesions are generally benign and complete surgical excision leads to biochemical remission and increased bone mineralization.
Footnotes
Authors’ Note
P.N. and M.C.T. contributed to drafting of manuscript and collection of data. N.L. and A.M.V. contributed to critical revision, supervision, and intellectual content of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.