
Abstract

Case Presentation
A 74-year-old female patient was seen at our department for a 3-month history of slowly progressive, painless, and bilateral neck swellings. Her relevant medical history was unremarkable, while her sociogram included a 55-pack-year history of smoking. Clinical examination revealed solid and well-defined neck masses located in the upper thirds of the neck bilaterally, measuring 10 and 25 mm on the right and left side, respectively. Apart from the size, both masses were similar in clinical appearance, nontender, mobile, and with intact overlying skin. Mirror laryngoscopy revealed chronic edematous laryngitis with preserved mobility of the vocal folds, while the rest of the clinical examination was unremarkable. A neck ultrasound demonstrated 2 oval, nonhomogenous, hypoechoic level 2A lymph nodes located on both sides of the neck, with diffusely enhanced vascularization and without visible hilums. Based on the clinical and ultrasonographic findings and the patient’s smoking history, a panendoscopy with the left-sided neck mass excisional biopsy was performed (Figure 1A and B). No endoscopic evidence of suspicious mucosal changes in the upper aerodigestive tract was noted and the histopathologic examination demonstrated the features of Warthin’s tumor. The immediate postoperative period was uneventful, and based on the benign characteristics of the excised lesion, we adopted the watchful waiting strategy for the contralateral neck mass. However, 3 months after the surgery, the patient came to our department with sudden and progressive enlargement of the right-sided neck mass noted on the initial examination. Based on the patient’s history, the presumptive diagnosis of another extraparotid Warthin’s tumor was made, and excisional biopsy in general anesthesia eventually confirmed the diagnosis (Figures 1C and D and 2). The patient is currently under regular checkups by the attending surgeon and has no recurrence over the 6-month follow-up.

A and B, A well-defined and encapsulated tumor exposed through the left-sided transverse cervical incision approximately 3 cm below the angle of the mandible. The tumor is clearly located in the neck, without the involvement of the parotid tissue. C and D, A contralateral tumor exposed through a similar incision. The tumor showed an increase in size from 10 mm on initial examination to its current size (25 mm) at the time of second surgery.
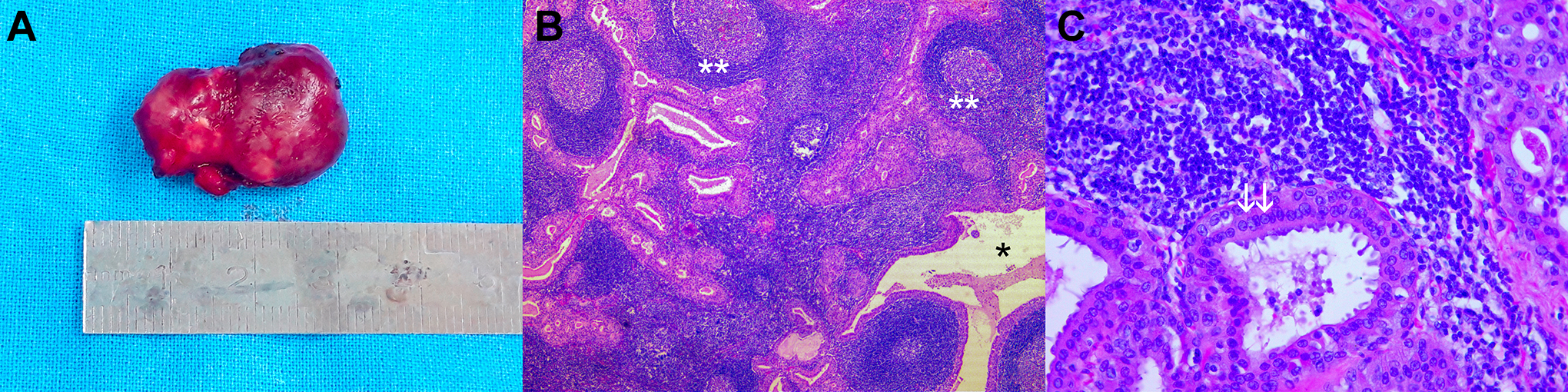
A, Macroscopic appearance of the excised right-sided lesion. The tumor is well demarcated and surrounded by a thin capsule. B, Histopathologic features of the excised right-sided tumor. The tumor consists of multiple cystic spaces surrounded by bilayered oncocytic epithelium (*) and a lymphoid stroma (**) with varying degrees of reactivity and formation of germinal centers (H&E, ×50). C, The epithelium demonstrates 2 distinct layers of cells: tall and columnar luminal cells and cuboidal basal cells (H&E, ×400).
Discussion
Warthin’s tumor (adenolymphoma, papillary cystadenoma lymphomatosum) is a benign salivary gland tumor typically found in the parotid gland, accounting for up to 30% of parotid neoplasms, second only to pleomorphic adenoma.1-3 Unlike other parotid tumors, bilateral or multifocal lesions are not uncommon, and extraglandular localization of the tumor in the neck lymph nodes has been reported as well.3,4 Although the exact pathogenesis of Warthin’s tumor is uncertain, there seems to be a strong association with tobacco smoking, with smokers reported having 2- to 8-fold increased risk for developing the disease.5,6 The late encapsulation of the parotid gland during the embryogenesis allows the mixing of developing lymphoid tissue with the salivary parenchyma, which eventually results in the presence of ectopic salivary ducts and acini within the intra-, periparotid, or laterocervical lymph nodes. It is suggested that Warthin’s tumors develop as a result of the neoplastic proliferation of these ectopic salivary elements in the lymph nodes.5,7 The typical clinical finding of Warthin’s tumor is of a slowly growing and asymptomatic parotid tail mass. Extraparotid lesions located in the neck may clinically and radiologically mimic the metastatic lymph nodes, especially in the event of rapid enlargement, as in our case. The suspicion of metastatic disease from the head and neck primary is further emphasized by the fact that most patients are male smokers in their 6th and 7th decade of life, although recent studies demonstrate a more balanced disease distribution between genders. 6 The diagnosis of extraparotid Warthin’s tumor is challenging and is often confirmed only after the excisional biopsy of the suspicious lymph node. Fine needle aspiration cytology (FNAC) as an initial step in the evaluation of a neck mass may give misleading or inconclusive results and is often dependent on the institution or the experience of the cytologist. 8
While unilateral extraparotid Warthin’s tumors are best managed by simple local excision, there is no clear consensus on the optimal treatment of the bilateral lesions. If the diagnosis is eventually confirmed by FNAC, initial bilateral surgery may be performed. However, even if the bilateral disease is evident from the cytologic findings, some authors advocate the watchful waiting approach for the less involved side of the neck to reduce the postoperative morbidity, due to the benign nature of the disease and the extremely low potential for malignant alteration.9,10
Extraparotid Warthin’s tumor should be considered in the differential diagnosis in a patient with bilaterally enlarged cervical lymph nodes and especially without a clinically or endoscopically evident primary head and neck malignancy. If the diagnosis of extraparotid Warthin’s tumor is obtained after the excisional biopsy of the lesion on one side of the neck, a wait-and-see policy can be adopted for the contralateral tumor.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.