
Abstract

Lymphatic malformations (International Society for the Study of Vascular Anomalies classification), traditionally called lymphangiomas, are diseases caused by development errors of the lymphatic system. 1 Lymphatic malformations would grow rapidly with infection, trauma, or bleeding. 1 Pathologically, lymphatic malformations can be divided into 2 types: macrocystic (>1 cm, the most common) and microcystic (<1 cm), but mixed (macro- and microcystic) forms are usually present clinically.1,2 Lymphatic malformations occur commonly in children, and about 90% of the cases occur within 2 years of age.1,2 There is no gender preference. 1 Head and neck lymphatic malformations are rare, with incidence between 1.2 and 2.8 per 1000. 2 As minimally invasive surgery, we report endoscopically assisted resection of a cervical multicystic lymphangioma in an adult.
A 43-year-old female was referred to our hospital with a left cervical painless swelling. She had no previous history of trauma and infection. Contrast-enhanced computed tomography (CT) revealed a smooth-bordered, nonenhancing, unilocular, homogenous, and low-density cystic lesion (36 mm × 29 mm) was located in the anterolateral side of the sternocleidomastoid muscle and in the posterolateral side of the submandibular gland (Figure 1). Magnetic resonance imaging showed a well-circumscribed, heterogeneous, multicystic lesion (33 mm × 26 mm × 58 mm) with high signal intensity on T2-weighted image (Figure 1). Three-dimensional visualization of the relationship between cervical cystic lesion and related vessels was shown by CT angiovenography (Figure 1). Radiological diagnosis was multicystic lymphatic malformation. The patient underwent endoscopically assisted resection of the lesion under general anesthesia as minimally invasive surgery. A 2-cm incision on the skin was made (Figure 2), and the lesion was exposed after incision of the platysma muscle. Soft tissues surrounding the lesion were dissected, and a 30°, 4-mm-diameter, endoscope with tissue retractor (Karl Storz) was inserted into the wound (Figure 2). The lesion was dissected carefully with preservation of the facial artery under endoscopic guidance (Figure 2). The lesion was removed completely through the small skin incision, and wound was closed (Figure 2). Pathological diagnosis was lymphatic malformation (Figure 3). Postoperative course was uneventful, and there was no recurrence 5 years after surgery.
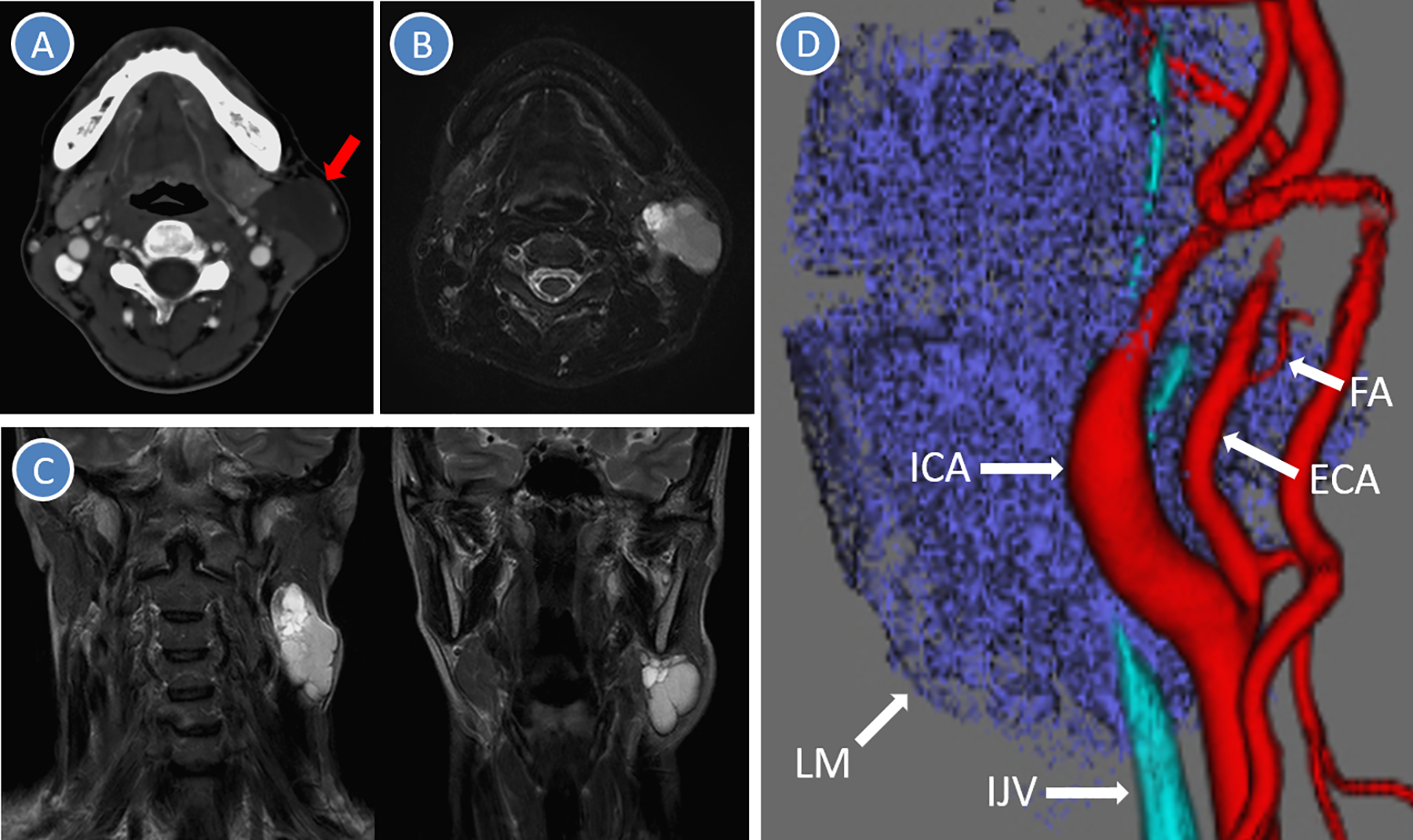
Computed tomography (CT) and magnetic resonance imaging (MRI). A, Contrast-enhanced CT revealed a smooth-bordered, nonenhancing, unilocular, homogenous, and low-density cystic lesion (arrow) was located in the anterolateral side of the sternocleidomastoid muscle and in the posterolateral side of the submandibular gland. B and C, Magnetic resonance imaging showed a well-circumscribed, heterogeneous, multicystic lesion with high signal intensity on T2-weighted image. D, Three-dimensional CT angiovenography. ECA indicates external carotid artery; FA, facial artery; ICA, internal carotid artery; IJV, internal jugular vein; LM, lymphatic malformation.
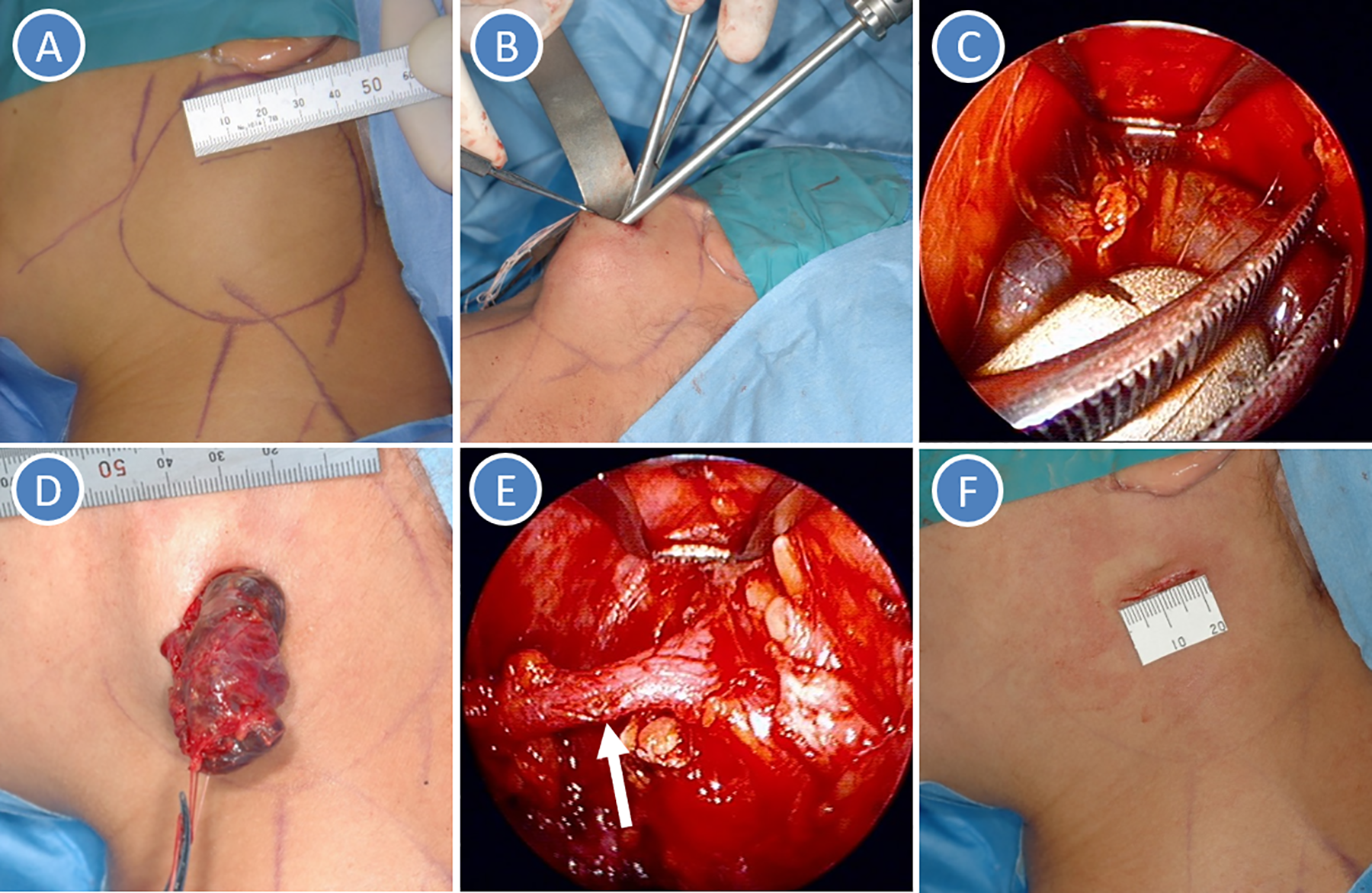
Surgical view. A, A 2-cm skin incision. B, Insertion of endoscope in the wound. C, Dissection of the cystic lesion under endoscopic guidance. D, Resection of the lesion. E, Preservation of facial artery (arrow). F, Wound closure.
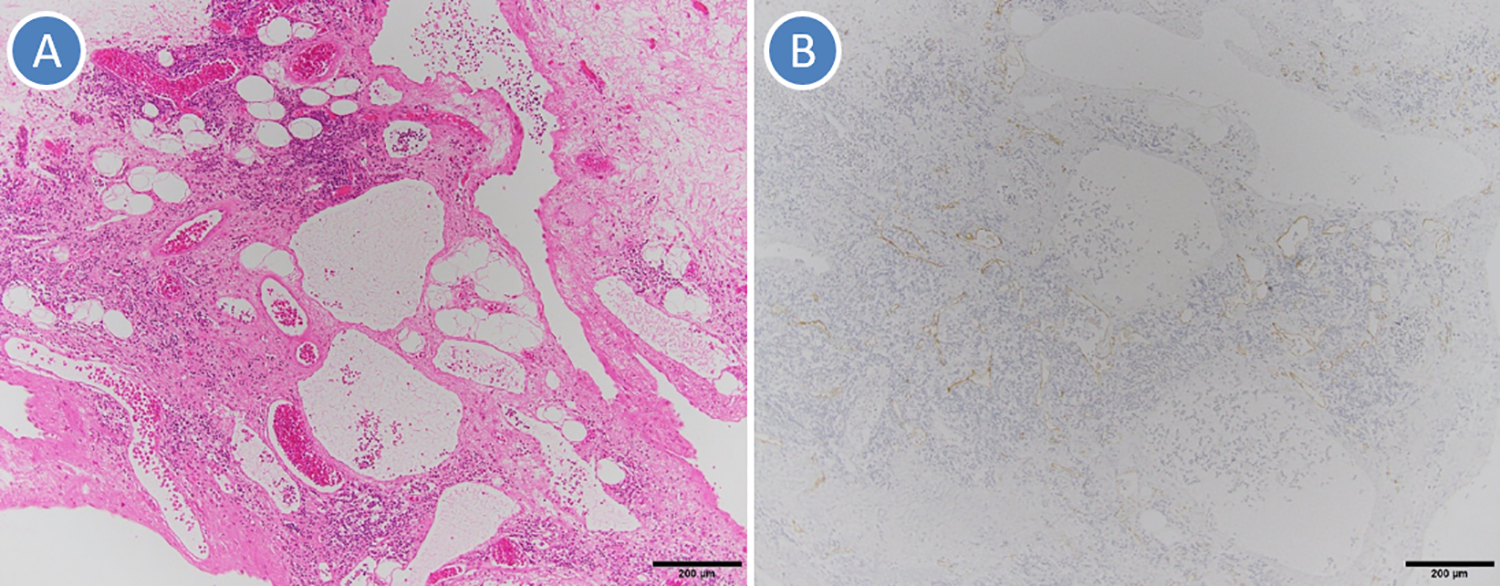
Pathology. A, The lesion is composed of dilated lymphatic vessels (H&E staining). B: Immunohistochemically, the endothelial cells of the lymphatic vessels show positivity to D2-40.
Surgery, sclerotherapy, laser therapy, and their combination are currently the treatment modes of lymphatic malformations. 1 Surgery is the main treatment for macrocystic lymphatic malformations, and other methods such as observation, sclerotherapy, radiation, hormone therapy, and aspiration are usually reserved for single room cysts or poor surgical candidates. 3 Cervical cystic lymphatic malformations often adhere to the carotid sheath, including the important vessels and nerves. 3 Therefore, preoperative imaging is very important for understanding the relationship between cystic lesions and vital anatomical structure and avoiding complications. 4 In the present case, 3-dimensional visualization of the both relationship was shown by CT angiovenography. Surgical resection should be performed after comprehensive evaluation of cosmetic aspects, prognosis, functional prognosis, resectability, and possibility of recurrence/complications. 5 Although cervical cystic lesions have traditionally been resected through an incision over the entire protruding zone for potential risks of recurrence or complications, endoscopically assisted neck surgery with preferable cosmetic outcome has been recently applied to cervical cystic lesions as minimally invasive surgery.3,4,6 However, endoscope without tissue retractor requires repeated cleaning of the tip during surgery. In contrast, the tissue retractor mounted to the endoscope can make surgical space and keep tip of endoscope clean.
Endoscopically assisted resection of cystic lymphatic malformation is minimally invasive, safe, and feasible treatment with better aesthetic results, but this surgery has technical difficulty and are time-consuming procedure. Therefore, selection of treatments should depend on the patient’s individual status and available technology and expertise.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.