
Abstract

Case Report
A 46-year-old woman was referred to our department after presenting to a local clinic with recent onset of intractable otorrhea and otalgia by topical treatment. She was referred to our department. History taking revealed that she had undergone tympanomastoidectomy 15 years ago in other hospital. She had experienced intermittent headaches for the previous 11 years that were controlled by medication. Magnetic resonance imaging (MRI) performed twice revealed no significant findings. Otoendoscopy findings showed intact neodrum without perforation. There was no granulation tissue within the external auditory canal. The pus culture and sensitivity test revealed no growth microorganism. Pure-tone audiometry revealed left-sided conductive hearing loss with bone conduction of 20 dB and air conduction of 35 dB under a conventional 3-frequency average. Temporal bone computed tomography reveals curvilinear radiopaque material along with dense soft tissue in the left mastoid cavity without opacification of the previous canal wall-up mastoidectomy site (Figure 1). The otorrhea was stopped by diluted vinegar irrigation with ototopical ciprofloxacin drop. Based on these examination findings, we planned endoscopic revision tympanoplasty with mastoidectomy. The surgery was performed under local anesthesia. Using an endoscopic approach, a tympanomeatal flap elevation was performed. The left tympanic membrane was lateralized, detached from the handle of malleus, and released from the promontory that was adhered to by fibrous tissue. The ossicle chain was intact. Through the antrum and attic, a mastoidectomy was performed. Foreign body material resembling cottonoid surrounded by granulation tissue was identified and removed (Figure 2). The tissue was sent for pathological examination. The tympanomeatal flap was adjusted, and nylon mesh and Merocel packing was performed using the rosebud technique. The pathological examination of the foreign body and granulation tissue showed foreign body material with fibrosis. A high-power microscopic examination demonstrated multinucleated foreign body giant cells (Figure 3).
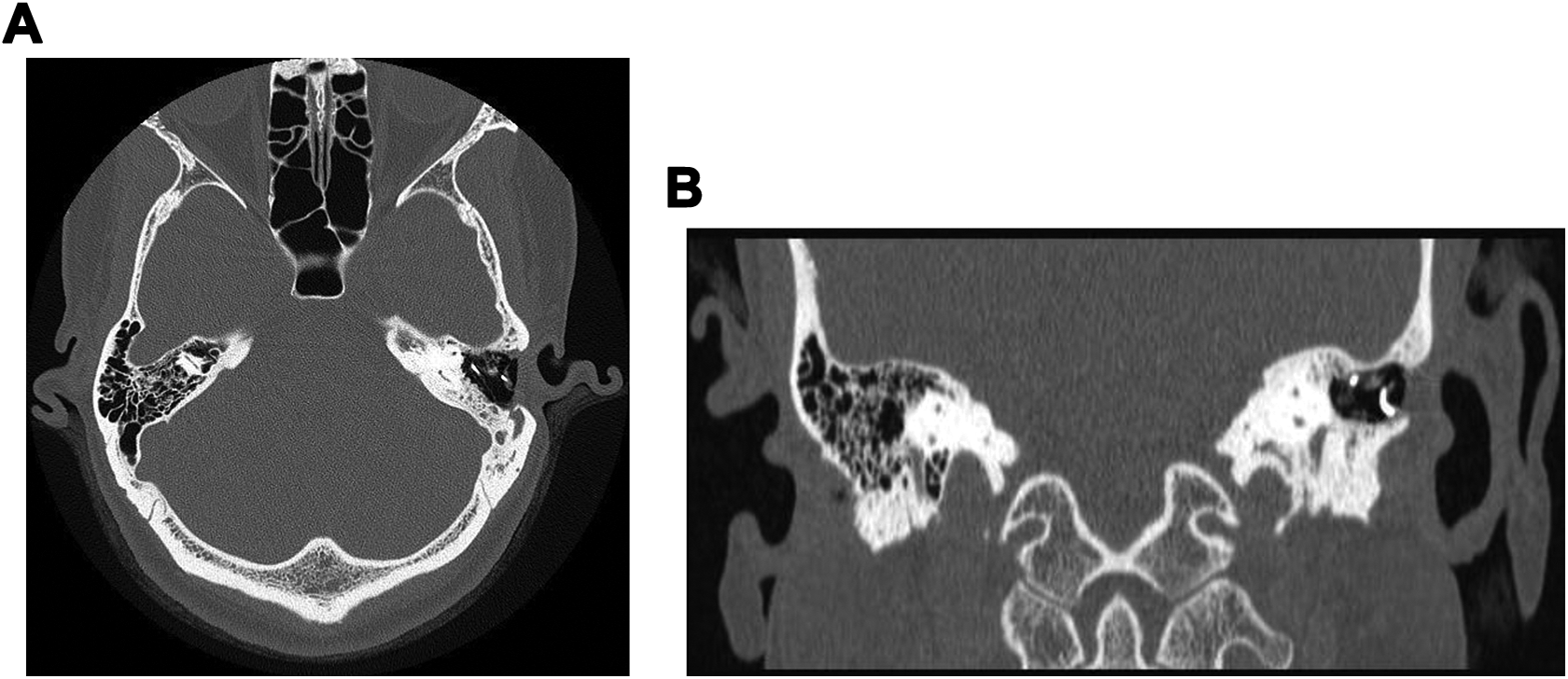
A, Axial unenhanced computed tomography (CT) image showing dense hyperattenuated metallic filaments without opacification of the mastoidectomy cavity. B, Coronal unenhanced CT image showing the characteristic curvilinear metallic density with a dense soft tissue.
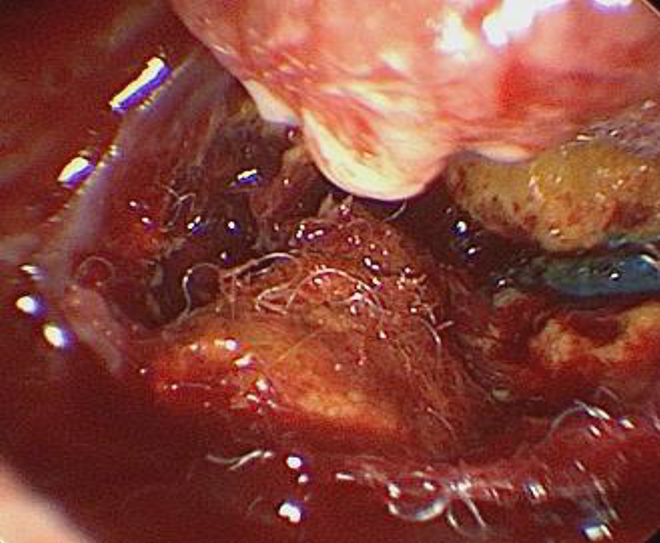
Intraoperative endoscopic image showing foreign body material suggestive of cottonoid surrounded with granulation tissue in the mastoid cavity.
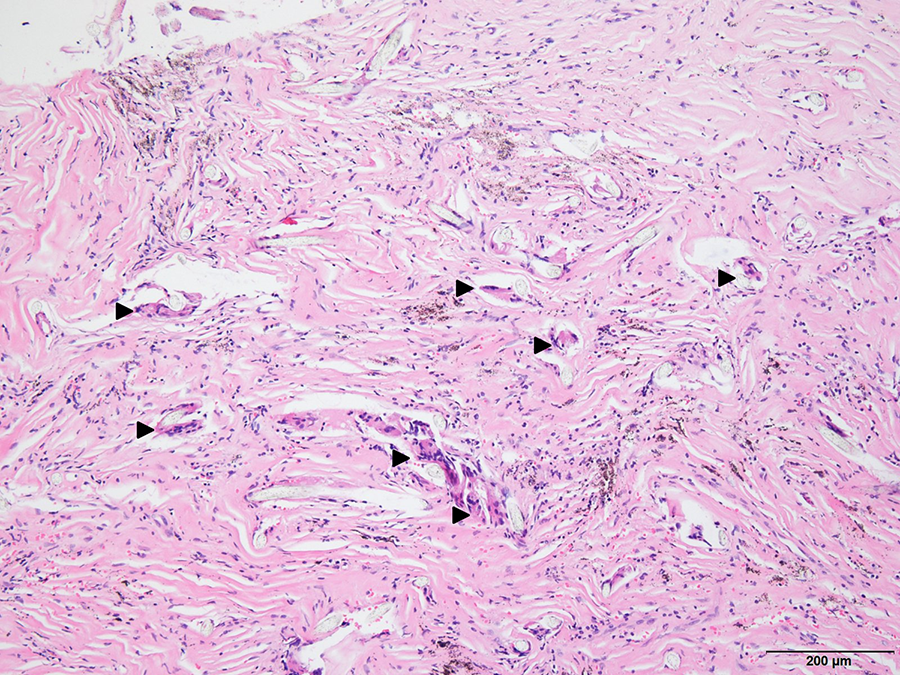
Pathologic image showing multinucleated foreign body giant cells (arrowhead). H&E stain, ×100.
Discussion
A few studies of gossypibomas, the most accepted term for “retained surgical sponge,” have been published, mostly in cases of abdominal and pelvic surgery.1,2 Despite a reported incidence of gossypibomas of 1 in 100 to 3000 of all surgical interventions, cases are rarely reported in head and neck surgery. The only case report of retained surgical cotton sponge in microscopic ear surgery was published in 1954. 3
Although difficult to diagnose by otoendoscopic examination, nonresorbable cottonoid surgical sponge has a radiopaque barium sulfate monofilament marker, which is readily visible on temporal bone CT and on plain radiographs. 1 These filaments appear as curvilinear hyperattenuated structures. Due to the history of intermittent headache, the patient underwent an MRI twice prior to visiting the otorhinolaryngology department. The radiologists found no significant abnormality. Since barium sulfate is a proton-poor compound, it is generally not detectable on MRI. 2 Magnetic resonance imaging is more useful when the foreign body reaction appears as a mass lesion. 4 Few reports of MRI described a retained sponge as a dense soft tissue mass with a thick and well-defined capsule.2,5 Another study reported whorled stripes with a central low-signal portion on a T2-weighted image. 6 The patient showed a low signal on T2-weighted image in both previous MRI studies suggesting fibrotic tissue with no fluid.
A mastoidectomy while removing the foreign body and the surrounding granulation tissue was sufficient for complete treatment. One study showed that the longer the retention time, the higher were the risk of complications, such as an increase in fistula formation in other body parts. 7 However, even though the foreign body material had been in the patient for 14 years, she had experienced otorrhea and otalgia but no perforation or erosive lesions on the external auditory canal. In a prior case report published in 1954, the patient carried foreign body material for 32 years but recovered fully from vertigo and otorrhea postoperatively. 3
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.