
Abstract

Report of Case
A 13-year-old boy was referred for recurrent epistaxis and worsening obstructive sleep apnea symptoms over a 6-month period. computed tomography and magnetic resonance imaging demonstrated a large, left-sided mass of the nasopharynx extending into the maxillary sinus and pterygomaxillary space to the orbital apex (Figures 1 and 2). He subsequently underwent tumor embolization followed by combined endoscopic transnasal and transantral removal of the tumor and was discharged on postoperative day 1. He has had no surgical complications and no evidence of recurrence after 5 years.
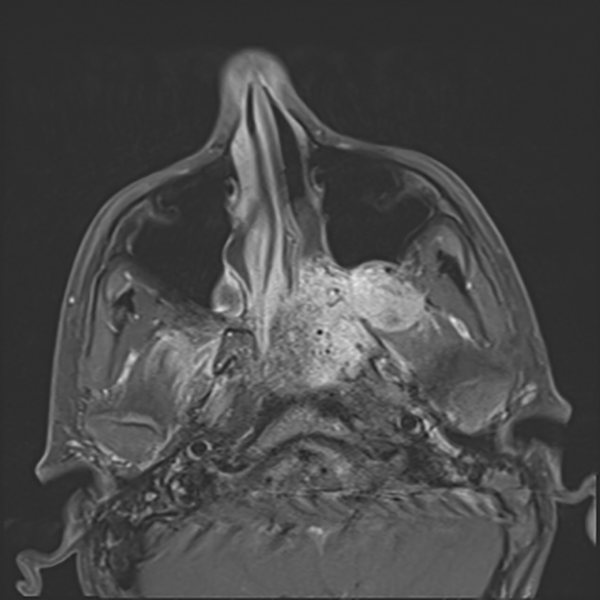
T1-weighted magnetic resonance imaging (MRI) image of left-sided nasopharyngeal tumor.

Coronal computed tomography (CT) with contrast showing tumor extending through an expanded sphenopalatine foramen.
He presented to a pediatric gastroenterologist at age 17 years for suspected gastroesophageal reflux and abdominal pain; due to a strong history of familial adenomatous polyposis (FAP) in his mother and multiple relatives, he was taken for upper and lower endoscopy. He was found on esophagogastroduodenoscopy to have greater than 10 polyps and more than 60 polyps on colonoscopy. Genetic testing revealed a heterozygous adenomatous polyposis coli (APC) mutation (c.453delA; p.Glu152LysfsX18). He ultimately underwent total proctocolectomy, which revealed multiple tubular adenomas throughout the length of colon ranging from 0.2 to 1.2 cm in greatest dimension.
Discussion
Familial adenomatous polyposis is an inherited autosomal dominant disease due to a defect in the APC gene and accounts for around 1% of colorectal cancers. The disease is usually diagnosed in adolescence but can present as late as the mid-30s and may be highly variable between members of the same family. Approximately 30% of individuals with an APC-related condition are found to have a de novo variant; in these instances, a patient’s family history would not be suggestive of this condition, and diagnosis is often delayed until a manifestation arises. In the classic presentation, numerous adenomas, ranging from 100 to 1000, are initially observed and prophylactic colectomy is recommended to prevent inevitable transformation into colorectal cancer. Not only does this disease affect the colon but patients can have extracolonic manifestations such as fundic gland polyps in the stomach (as observed in our patient), fibromas, hepatoblastoma, and desmoid tumors. 1 Guertl et al were unable to detect APC mutations in 9 patients with Juvenile nasopharyngeal angiofibroma (JNA) and therefore suggested that JNA may be an extracolonic manifestation of FAP 2 caused by a gene other than APC. On literature review via PubMed, there have been less than 10 cases reported of patients who have JNA and FAP, and some have doubted the link in population studies. 3
Juvenile nasopharyngeal angiofibroma is a highly vascular neoplasm that solely affects adolescent males and makes up 0.05% of total head and neck tumors. 4 Even though this neoplasm is relatively rare in the general population, in certain series it is 20 to 25 times more prevalent in the FAP population than in age-matched controls.5,6 The exact mechanism of JNA is not completely understood; however, an androgen-driven pathogenesis is suspected due to its predilection of adolescent males. 2 Estrogen-driven desmoid tumors of women who have FAP appear during childbearing years, and this may happen in a similar manner to JNA. 6 As previous reports have identified germ line APC variants in individuals with JNA at an incidence greater than expected for individuals of the general population and somatic alterations within JNA, this association has been proposed.
Juvenile nasopharyngeal angiofibroma may be one of the first manifestations of FAP, with patients presenting in early teenage years prior to developing gastrointestinal symptoms. This pattern was a common finding in the literature. 7 Therefore, it is important for otolaryngologists to consider FAP as an underlying diagnosis especially in patients who have a family history of FAP or colon cancer.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.