
Abstract
We report a case of a 13-year-old boy presented with left facial nerve paralysis (Figure 1). Ten months ago, he complained of progressive increase in hearing loss in the left ear with intermittent discharge. He also had lifelong recurrent symptoms of chronic otomastoiditis in the left ear. A series of investigations were carried out immediately upon his presentation to the Ear, nose and Throat (ENT) clinic. This included computed tomography (CT) scan of the head and neck which showed left middle ear and mastoid cavity occupied by soft tissue mass eroding the internal acoustic meatus (IAM content). Soft tissue opacification was seen in the middle ear to the extent that the ossicles were not visualized. The mass caused destruction and erosion of the left mastoid bone with infection of the vestibule and cochlea, creating a boundary separating the internal auditory canal from the opacified middle ear cavity. Bone destruction was observed in the anterior and posterior part of the mastoid bone with connection of the ear cavity. Unfortunately, the lesion extended to the IAM and left facial canal causing left facial nerve paralysis (shown in Figure 2). The differential diagnosis was left ear cholesteatoma versus left ear neoplasm. Importantly, histological and microbiological studies showed amorphous brownish grain-like material with eosinophilic edges and septal hyphae at its core. This led to the diagnosis of eumycetoma of the left ear. Pure-tone audiometry showed severe hearing loss in the left ear and normal right ear function. Radical surgery with exploration of the mastoid cavity and middle ear under magnifying microscopic was carried out. Under the operating room microscope, black debris was found and totally removed (Figure 3). The IAM defect was sealed by cartilage grafting and fascia, and they were placed closed to the IAM defect and fixed by glue and gel foam; no more leakage was observed 6 months after the operation. The parent gave consent for publication of the case report.

Ear mycetoma in a 13-year-old boy presented with left facial nerve paralysis.
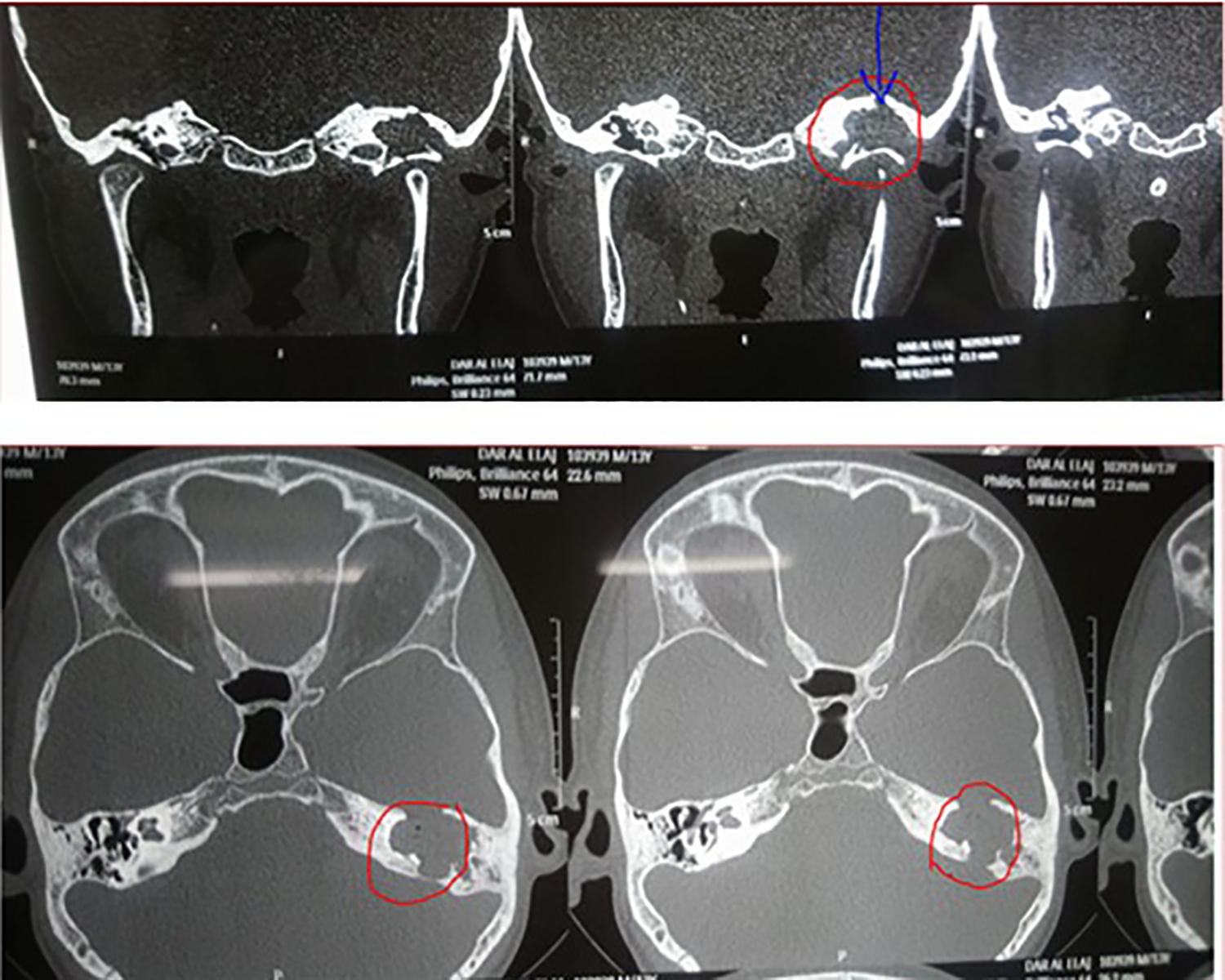
Computed tomography scan of the temporal bone showing tissue mass occupying the left middle ear and mastoid cavity causing destruction and invading the internal acoustic meatus.

Mycetoma black grains which were removed from the ear, mastoid cavity, and internal acoustic meatus.
Mycetoma is a rare disease of the poor populations and known to be associated with high mortality and morbidity in endemic area especially in childhood.1-3 Mycetoma is a chronic infection and can be due to fungi (Eumycetoma) or bacteria (Actinomycetoma). Sudan is part of the mycetoma belt, which includes other countries such as Somalia, Senegal, Mexico, and India. 4 The infection occurs following the introduction of causative organisms through the skin due to a minor trauma or injury from sharp thorn (soil is common inhabitant of the organism). Once the organism is introduced into to the skin, it leads to formation of granulomatous inflammation that causes painless swelling of the foot and leads to the invasion of the muscles and bones. 5 The inflammation is associated with formation of sinus that leads to intermittent or regular serous, serosanguinous, or purulent discharge. The discharge during active disease can be associated with granules of different colors (black, red, or white). Black granules are likely due to Madura mycetomatis. 5 Males are more likely to have the infection, and the most common age is 15 to 30 years old. Diagnosis of mycetoma will require different modalities of investigations such as CT scan, magnetic resonance imaging combined with histology, and fine needle aspiration. 5 Despite the fact that the most common site of infection is foot, mycetoma can affect different parts of the body including head and neck. Fahal et al described the presence of head and neck mycetoma in 49 patients. 6 To our knowledge, this the first case report of mycetoma in the left ear with invasion of the IAM, in Sudan.
Head and neck mycetoma was reported in several case reports and was attributed to different fungal infections. For instance, Moniot et al reported a case of malignant otitis externa (MOE) with jugular vein thrombosis caused by mycetoma that linked to Aspergillus flavus. 7 Yao and Messner also reported MOE in patients with HIV, and it was attributed to fungal infection called Scedosporium apiospermum. 8 Interestingly, Chhangani et al reported about mycetoma of the middle ear cleft 4 decades ago. 1 It worth mentioning that among the 49 patients with head and neck mycetoma reported by Fahal et al, 6 none of these patients have similar clinical presentation to the patient presented in this case report (left facial nerve palsy, deafness, discharge from the left ear, and the presence of the black grain). The presence of black debris and the excellent response to antifungal medication may suggest that the infection was likely due to Madura mycetomatis. The most infected site was lower extremity especially Madura foot, while a few other sites have been reported in toe of foot, right thigh, head, neck, oral cavity, breast, and chest wall.9-13 It will remain a puzzle to understand how he got the infection to his left ear. We postulate that our patient’s ear infection was inoculated with mycetoma infection following swimming in water colonized with mycetoma or activation of the fungal colonization was most likely due to the minor trauma of the ear following insertion of small piece of wood from local trees in order to clear ear wax or relief itchy sensation inside the ear canal. The latter can be common practice in rural areas in Sudan by adults. Sadly, such techniques may be used by many people in rural areas to remove foreign bodies in the ear.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.