
Abstract

A 40-year-old woman underwent a head computed tomography (CT; Figure 1A) at the emergency department of our hospital after a car accident which demonstrated a 2.2 cm × 2.0 cm oval lesion with a thick sclerotic margin in the sphenoid sinus. She had a 3-year repeated dizziness and intermittent moderate headache and “common cold” and initially deferred further workup. No positive findings were revealed on physical examination. Magnetic resonance imaging (MRI) demonstrated heterogeneous isointensity on T1- (Figure 1B) and hypointensity on T2-weighted fat suppression imaging (Figure 1C). The tumor was excised completely under rhinoscopic surgery, and the pathology specimen revealed polygonal mononuclear tumor cells (Figure 2A). Immunohistochemical staining which discovered on gastrointestinal stromal tumor 1 (DOG1; Figure 2B) confirmed the tumor as chondroblastoma (CB).

A, Computed tomography shows an oval lesion in the sphenoid sinus with a thick sclerotic margin with a scattered calcification in the mass. B and C, Magnetic resonance imaging preoperation shows an expansile lesion in the sphenoid sinus heterogeneously isointense on T1- and hypointense on T2-weighted fat suppression imaging
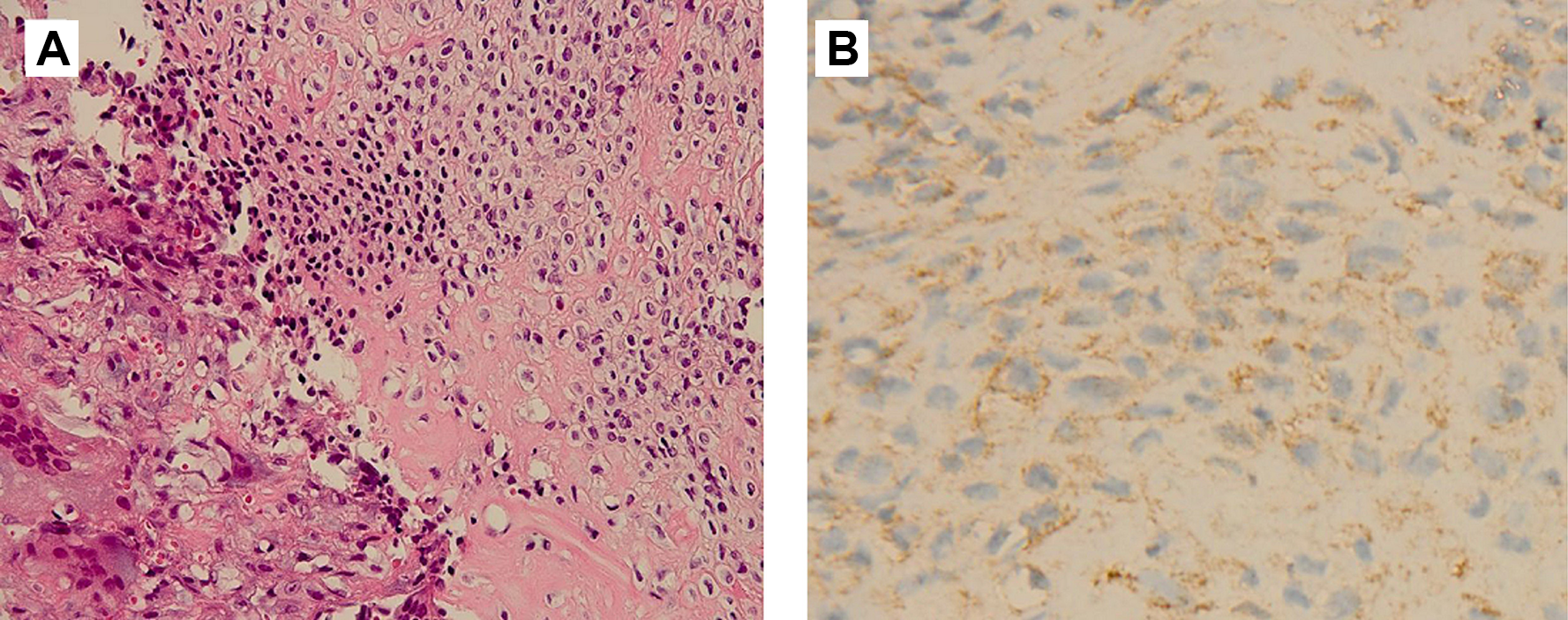
A, Tumor tissue section on H&E shows osteoclast-like giant cells and polygonal mononuclear tumor cells with well-defined cytoplasmic borders. B, Tumor tissue section on discovered on gastrointestinal stromal tumor 1 (DOG-1) shows part of the tumor cells moderately positive for DOG1.
Chondroblastoma is a rare tumor accounting for less than 1% of all primary bone tumors, commonly localized at the epiphysis or apophysis of long bones with prevalence in the first 2 decades of life and male predominance.1-3 It is rare in the head and neck with temporal bone as the frequent originating site and occurs in the fourth and fifth decade, which is significantly older than for long bone CB. 3 Only 3 cases have been reported in the sphenoid sinus.4-6 The differential diagnosis includes chondromyxoid fibroma, giant cell tumor, chondrosarcoma, eosinophilic granuloma, and noninvasive fungal sinusitis. 3 Chondroblastoma originated in paranasal sinus is hardly detected in the early stage for the lack of positive clinical presentations. Chondroblastoma on CT imaging is characterized by oval mass with a sclerotic rim and scattered calcification inside the lesion.2,3 On MRI, lesions appear T1 heterogeneously isointense and T2 hypointense on fat suppression imaging.2,3 Histologically, polygonal mononuclear tumor cells with well-defined cytoplasmic borders, a fine network of pericellular calcification (“chicken-wire” pattern), and immunohistochemically positive staining with S-100 protein are the characteristics of CB.3,4 Immunostaining with DOG1 may help to confirm the diagnosis if tumors present with untypically radiological or histological manifestations.3,7 Although CB is intermediate and locally aggressive and rarely metastasizing, radical resection and regular follow-up is recommended to reduce and prevent local recurrence and distant metastasis of CB.
Footnotes
Authors’ Note
Informed consent was obtained from individual participant included in the study.
Acknowledgments
The authors wish to express their sincere thanks to Dr Feng Liu for his valuable assistance on this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.