
Abstract

Introduction
Since the conception of 3D printing in the 1980s, its technology and materials have improved, are less expensive, the expertise is more widespread, and therefore it has been available in many parts of the world.1,2 Several studies have explored the use of 3D printing technologies in medical education and more specifically in surgical training. Significant advantages are patient safety, favorable supervision in a less stressful environment, there is no need for cadaveric dissection equipment most of the times, cadaveric specimens can be saved, and the surgical procedures can be standardized and reproduced. An additional advantage is the haptic feedback that is more realistic compared to virtual reality applications.
We are aiming to present our experience in the development of an “in-house” myringotomy and grommet insertion simulator. The principal purpose of our attempt is to introduce a setting that can be adopted by any ENT department or individual based on low cost, simple setup, good reproducibility, and anatomical accuracy.
Materials and Methods
The model we used was printed in resin with the Selective Laser Sintering (SLS) methodology. Initially, a DICOM file of a computed tomography of the temporal bones was converted to .stl format. It consisted of 2 parts: one included the auricle and the external acoustic meatus (Figure 1) and the second included the middle ear cavity and the handle of the malleus (Figure 2). The rest of the ossicular chain was deemed unnecessary. Aiming to simulate the tympanic membrane, we used transparent film between the ear canal and the middle ear, resting on the handle of malleus (Figure 3). This allowed orientation and evaluation of the landmarks while adding stability during myringotomy. The hollow middle ear cavity allows the use of a fluid, simulating middle ear glue.
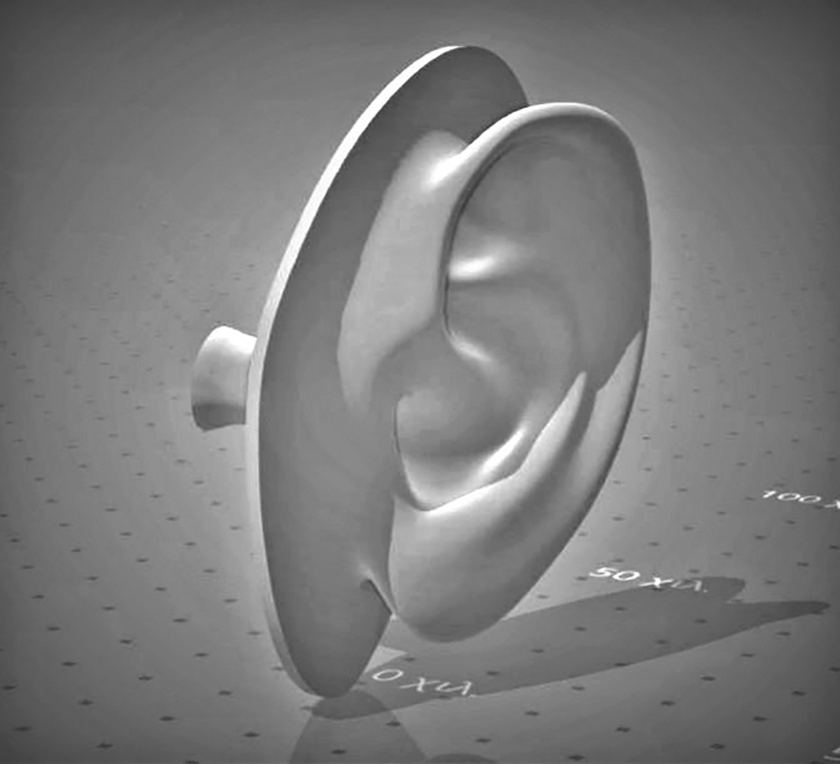
First part including the pinna and the external auditory meatus.
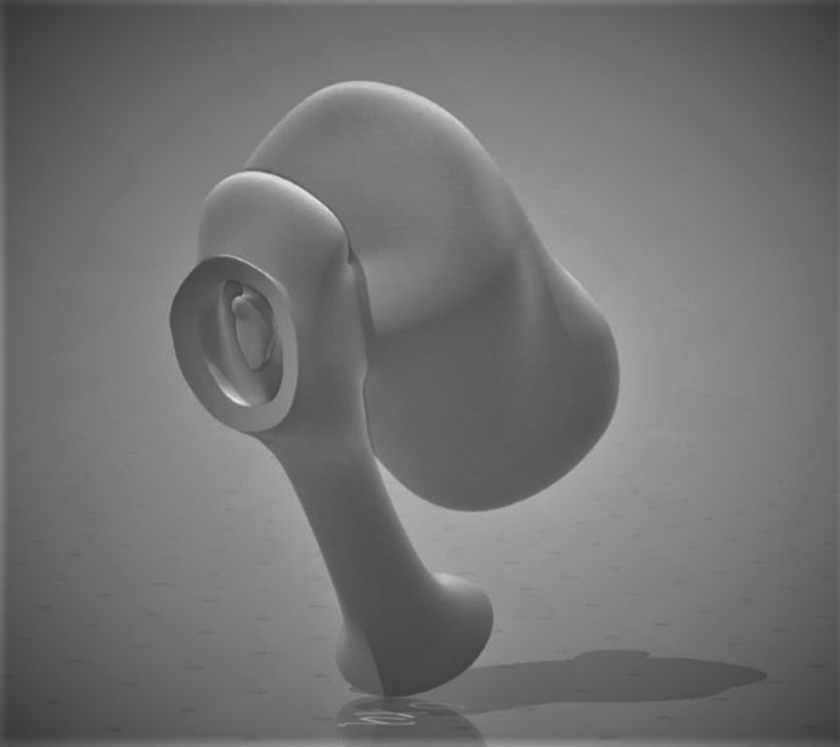
Second part including the middle ear cavity and the handle of the malleus.

Grommet inserted on the anteroinferior quadrant of the membrane.
Discussion
Canzi et al identified 23 studies in the literature focusing on otologic applications in training, mainly having to do with temporal bone surgery simulation. 3 Although there are models showing satisfactory reproducibility of most structures and anatomical landmarks, there are issues to be overcome such as the accuracy of the ossicular chain (mainly the stapes) and the retained resin within the middle ear and mastoid air cells. 4 We dealt with those issues by using laser sintering technology and resin as our material. On the other hand, it is still difficult to approach the “natural” structure of the cadaveric specimen, mainly due to the “stair-stepping” artifact and the lack of anatomical elements. 5 Hochman et al showed that tactile feedback is satisfactory by analyzing subjective and objective methods. The improvement in materials has provided a better simulation of bone consistency, resulting in a more realistic experience. 6 This is something we also realized, and we attribute this to the printing technology we selected.
Conclusions
Traditionally, myringotomy and grommet insertion training has been taught on cadaveric dissection setting or in the operating theater. The implementation of emerging 3D printing technology carries significant advantages and can lead to a new era in surgical simulation and training.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.