
Abstract

Introduction
Abscess of the tongue is a very rare disease.1,2 It is a potentially life-threatening clinical entity because elevation and backward displacement of tongue may compromise airway.3,4 Accurate diagnosis of these lesions has important prognostic and therapeutic implications. 1 When diagnosed, these lesions are opened and drained. Most tongue abscesses are unilateral and located in the anterior two-thirds of the tongue. 2 The etiology of tongue abscesses may differ depending on their location. In the posterior third of the tongue, abscesses most often originate as lingual tonsillar lesions, infected thyroglossal duct cysts, 4 ectopic thyroid gland, 5 or extensions of apical infections from the first or second molars. Although the diagnosis can be reached clinically, sometimes no specific sign or symptom is present, making the diagnosis difficult. 6
Case Report
A 42-year-old female patient with severe continuous pain and swelling of tongue for 15 days was presented to Unit of Otorhinolaryngology, Federico II University Hospital. The patient referred dysphagia, odynophagia, and speech difficulty but no dyspnea.
She denies history of smoking, any toothache or dental caries, having a good dental hygiene. The patient had no history of fever and chills, but she refers remote history of a previous tonsillitis.
On clinical examination, low-grade temperature elevation, significant swelling of the tongue, and drooling with painful lingual protraction were noted. The overlying lingual mucosa was intact. Palpation of the hyoid region and cervical anteflexion was painful. No trismus, lingual, or palatal tonsillitis was noted.
The nasofibroscopy showed a marked swelling of the posterior tongue that pushed down the epiglottis and prevented visualization of the vocal folds (Figure 1). The white blood cell count and the C-reactive protein were elevated.
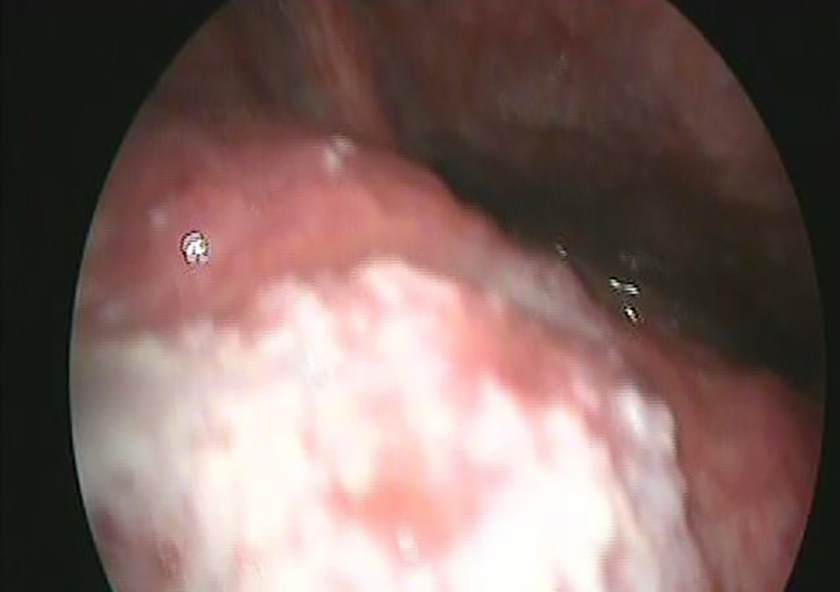
Clinical presentation of tongue abscess with a sharply bordered and superficially protruding painful mass lesion.
Computed tomography (CT) revealed an oval fluid density collection within the root of the tongue. No cellulitis or foreign body was visualized.
Magnetic resonance imaging (MRI) showed lesion of irregular configuration, multiloculated, measuring 4 × 4 cm at the base of the tongue, characterized by signal hyperintensity on T2-weighted sequences and signal hypointensity on T1-weighted sequences. The lesion presented peripheral enhancement after paramagnetic contrast, with intense edema and swelling. Fat-suppressed images helped to easily distinguish the involved tongue from the spared parenchyma (Figure 2).

A contrast-enhanced sagittal T1-weighted magnetic resonance (MR) image shows a diffuse intralingual lesion, located centrally, within the root of the tongue, bowing the genioglossus muscles. The lesion has a central area of low-signal intensity with peripheral high-signal intensity.
The patient underwent a ventral midline incision and drainage of the lingual abscess which produced 10 mL of purulent material. The procedure was performed under local anesthesia. The microorganism responsible for the abscess was Staphylococcus species and anaerobes grow on culture. The patient has improvement in the pain and the general state.
She was given Ceftriaxone 1 g/d for 10 days and Tachipirina 1000 orally once a day for 7 days. The fiber rhinolaryngoscopy showed a resolution in swelling of the tongue and a correct visualization of the vocal folds. Sagittal T1-weighted MRI study one month later confirms resolution of abscess changes (Figure 3).

Follow-up magnetic resonance imaging (MRI) sagittal T1-weighted image shows a normal tongue after one-month from drainage of the abscess.
Discussion
Lingual abscess is a rare potentially life-threatening clinical entity, often considered an emergency. 3 Despite exposure to many potential pathogens, tongue is comparatively immune to infection and an unusual site of abscess. Some of the reasons for this immunity include constant mobility of the tongue, which helps the saliva produce a perpetual cleansing effect; its thick covering of keratinized mucosa, which is not easily penetrated by microorganisms; the muscle tissue, which constitutes the chief bulk of its parenchyma, with its rich vascular supply; its rich lymphatic drainage; and the immunologic properties of saliva. 6 Tongue abscess frequently presents as painful swelling which causes protrusion of the tongue, dysphagia, odynophagia, and difficulty with speech.4,6 There are 2 forms of lesions by localization: superficial or deep abscess.
In superficial abscess, the inflammatory process is located directly beneath the mucous membrane. The main location is the back of the tongue. Patients complain of pain during talking, eating, and swallowing. A detailed examination is determined by the limited swelling and hyperemia in the tongue. It is dense, enlarged, painful during palpation. A pathological focus with such an arrangement can open and spontaneously drain on its own. After that, the patient feels a reduction in pain and a decrease in swelling. Although the tongue wound can quickly epithelialize, relapse of the abscess is possible without adequate treatment.
The deep abscess is characterized by the inflammatory process involving the deep muscle tissue of the tongue. The course is more severe, with fever of 38° to 39°, general weakness, loss of appetite, and headache appear.
An objective examination reveals a significant increase and swelling of the tongue. There is impairment of speech and food intake, the saliva becomes viscous. In severe cases, it is difficult for the patient to breathe through the mouth and even drink liquid. Submandibular lymph nodes usually grow rapidly, becoming painful, but mobile.
Several imaging techniques, including sonography, CT, and MRI, can be used to evaluate the tongue abscess. Sonographic examination of a tongue abscess revealed a hypoechoic lesion surrounded by a hyperechoic ring, but sonography is not always feasible because when the tongue is swollen, the patient may experience discomfort or acute pain if it is pressed. The advantage of sonography is its ability to provide a diagnosis of tongue abscess and guide needle aspiration simultaneously. 7 Computed tomography is more helpful in diagnosing tongue infectious processes. The CT soft tissue window is useful to identify abscess location. The bone window can identify tooth infection, mandible osteomyelitis, or submandibular duct calculus. 8
Magnetic resonance imaging allows a better visualization of soft tissue and avoids artifacts of the jaw and dental amalgam. Typically, abscess presents as a T1 hypointense–T2 hyperintense lesion surrounded by a T1 hyperintense–T2 hypointense rim that enhances diffusely after contrast injection.9,10 This diffuse or peripherally enhancing appearance can mimic invasive squamous cell carcinoma, mucoepidermoid carcinoma, 11 or adenoid cystic carcinoma, 12 although having a different clinical presentation.
Another important point of view is that MRI can distinguish abscess from cellulitis. The presence of a surrounding wall, perilesional edema on T2-weighted and postcontrast images, a halo on postcontrast images, and a central necrotic area are highly suggestive of abscess. In cellulitis, the soft tissue stranding and dermal thickening are diagnostic. The important distinction between tongue abscess and lingual cellulitis often cannot be made clinically. Tongue abscess will not resolve without proper incision and drainage, while incision and drainage of a tongue cellulitis clinically accomplishes nothing.
The successful treatment of tongue abscess begins with an accurate diagnosis and consists of airway maintenance, incision and drainage followed by appropriate antibiotic therapy that should be directed against Streptococci, Staphylococci, and Gram-negative anaerobes. Aspiration alone is often insufficient therapy, since persistent nidus of infection may lead to abscess recurrence, requiring consideration of repeated aspiration or incision and drainage.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.