
Abstract

Neurofibromatosis (NF) is an autosomal dominant neurocutaneous syndrome characterized by aberrant growth of tumors (neurofibromas, neuromas, and schwannomas) in the skin and the central nervous system. 1 Neurofibromatosis type 1 (NF-1) is characterized by cutaneous neurofibromas, café-au-lait spots, ocular hamartomas, and skeletal abnormalities. It occurs in the head and neck in 20% of cases. 2 Although patients with NF may develop neurofibromas of the recurrent laryngeal and phrenic nerves, they are uncommon. Particularly, simultaneous occurrence of vocal cord and diaphragmatic paralysis is extremely rare. We herein report the rare presentation of bilateral mediastinal NF-1.
An 18-year-old man presented with complaints of hoarseness of voice, choking while eating, and progressive exertional dyspnea for 2 weeks. He had cutaneous manifestations of NF-1 (cutaneous neurofibromas, axillary and inguinal freckling, and café-au-lait spots). There was no significant family history, and he had no pulmonary symptoms. On examination, the patient was conscious with stable vitals. However, bilateral lower neck masses were palpable and left vocal cord paralysis was confirmed by indirect laryngoscopy (Figure 1A). Chest roentgenogram revealed paralysis of the left hemidiaphragm (Figure 1B). Chest computed tomography (CT) with intravenous contrast disclosed a series of bilateral multiple low attenuation masses with well-defined rounded margins along the intrathoracic course of the phrenic and recurrent laryngeal nerves (Figure 1C and D). Chest CT revealed displacement of the trachea to the right side and a series of multiple low-density mediastinal masses along the left recurrent laryngeal nerve, as well as elevation in the left dome of the diaphragm suggesting left phrenic nerve involvement (Figure 1D). The mass in the right prevascular space was suggested to have originated from the right phrenic nerve. The tumor of the right vagus nerve was found posteromedial to the right innominate vein and lateral to the trachea. The tumor of the left vagus nerve was noticed between the left common carotid and left subclavian arteries (Figure 1C). The biologic assessment and determination of tumor markers were unremarkable; however, spirometry revealed that maximal inspiratory pressures were mildly reduced to 80% of the predicted value. Neurofibromatosis was diagnosed by biopsy of the subcutaneous nodules, neck masses, and mediastinal masses (Figure 2A).
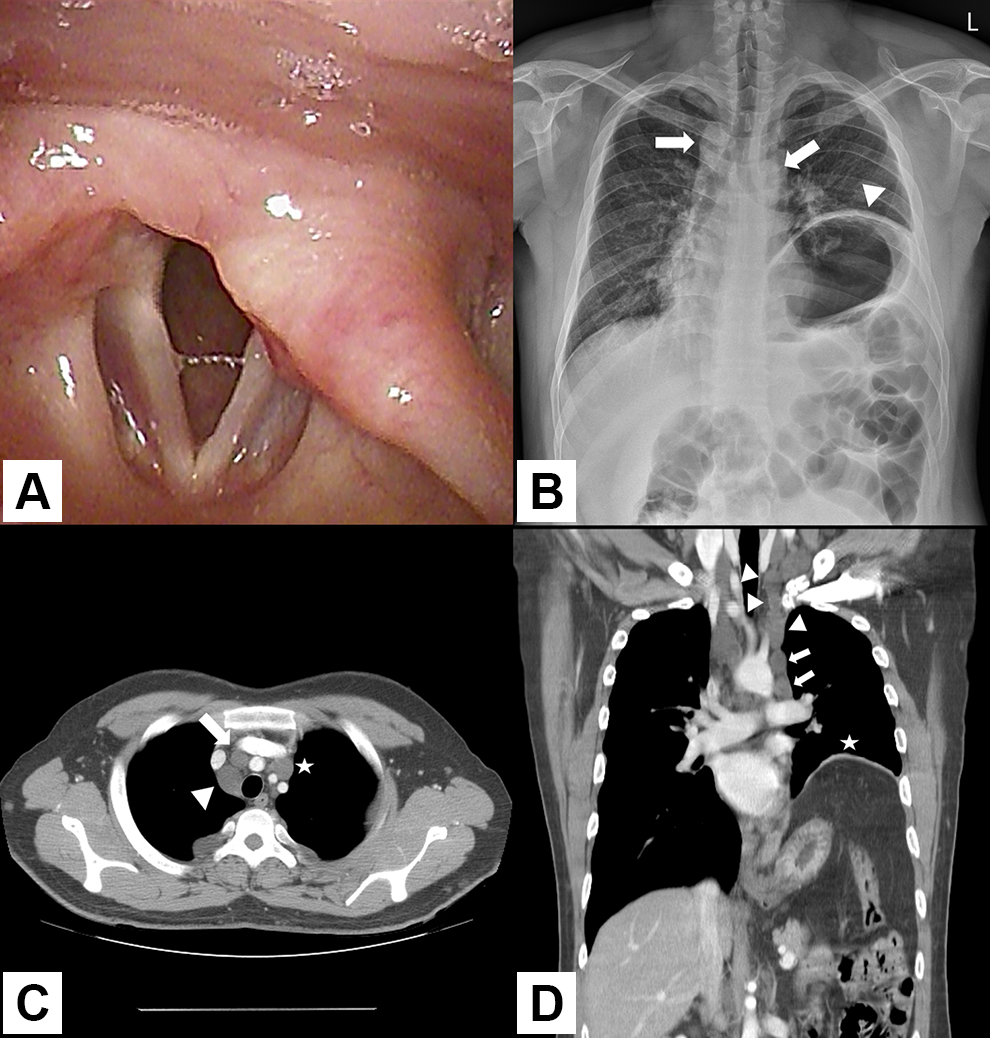
A, Left vocal cord paralysis observed on laryngoscopy. B, Chest roentgenogram anteroposterior view shows bilateral homogenous mass with well-defined rounded margins (arrows), as well as an elevated left hemidiaphragm (arrowhead). C, Axial computed tomography shows bilateral low-density mediastinal masses. The mass in the right prevascular space (arrow) may originate from the right phrenic nerve. The tumor of the right vagus nerve origin (arrowhead) is noted posteromedial to the right innominate vein and lateral to the trachea. The tumor of the left vagus nerve (asterisk) is seen between the left common carotid and left subclavian arteries. D, Coronal computed tomography shows a series of multiple low-density mediastinal masses along the left recurrent laryngeal nerve (arrows) as well as an elevated left hemidiaphragm (arrowhead).
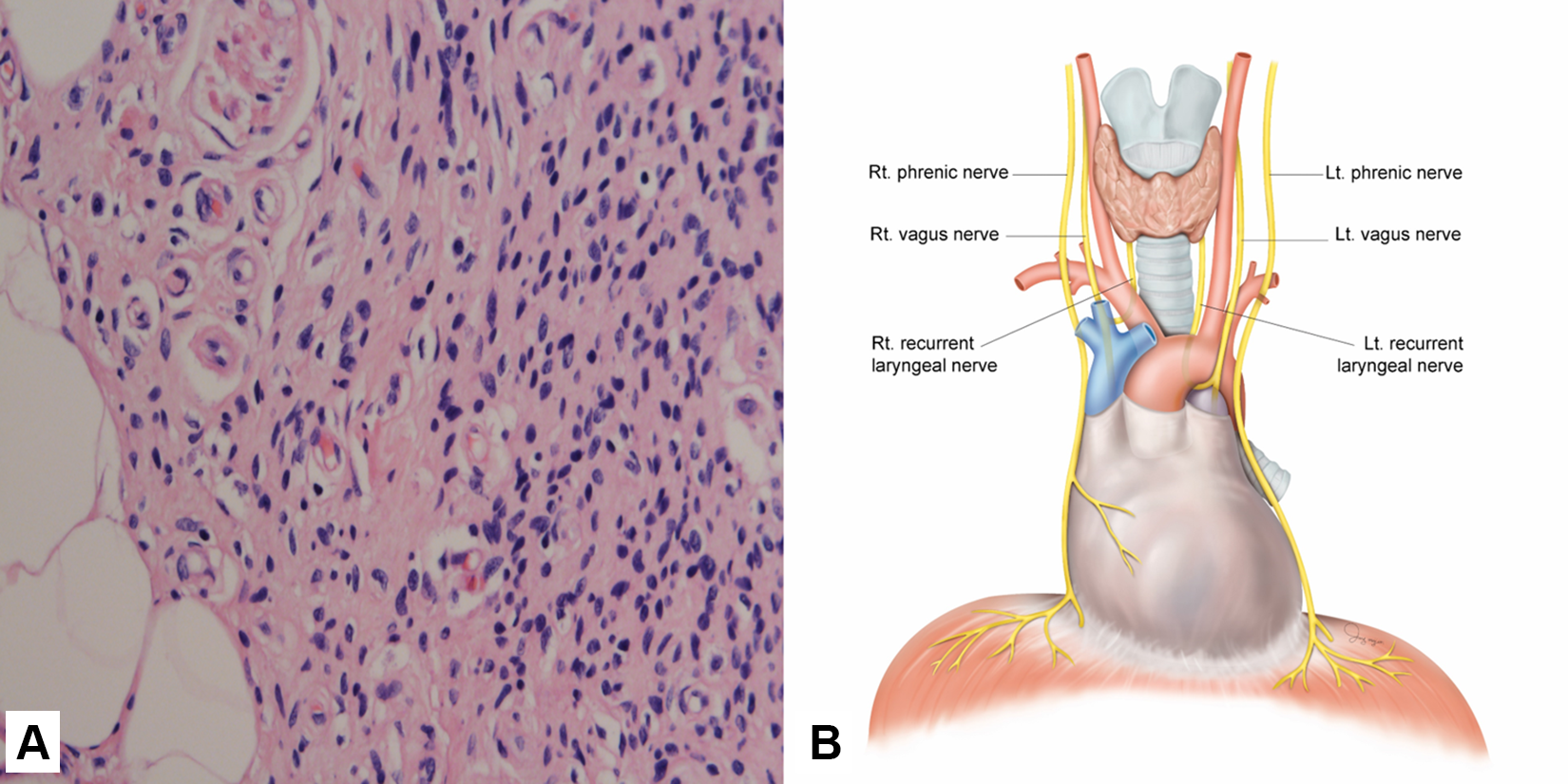
A, Histological examination showed spindle-shaped cells with narrow nuclei without atypia (hematoxylin and eosin, ×400). B, The course of both vagus and recurrent laryngeal and phrenic nerves.
Surgery is indicated for multiple tumors in NF-1 only in cases which are symptomatic, show enlargement of tumors, or undergo malignant degeneration. 1 Here, surgical intervention was suggested, but the patient was unwilling for surgery. At the 12-month follow-up, the patient was doing well, with no signs of worsening of symptoms.
Neurofibromatosis is a hereditary, autosomal dominant disease that affects approximately 1 in 3000 individuals. 3 Neurofibromatosis may present as a palpable neck mass or as a mediastinal mass on imaging. 1 We present an extremely rare case of intrathoracic neurofibromas originating from the phrenic and recurrent laryngeal nerves, which resulted in combined diaphragmatic and vocal cord paralysis. Here, unilateral phrenic and recurrent laryngeal nerve paralysis resulted in minimal morbidity, but in symptomatic cases with borderline lung function, diaphragmatic placation or surgical resection with a nerve graft seems effective. Although involvement of the phrenic and recurrent laryngeal nerves due to NF has been reported occasionally, 1 involvement of both the nerves simultaneously has never been reported. Patients with NF may present to an otorhinolaryngology clinic with various complaints such as hoarseness of voice, sleep apnea, stridor, and airway obstruction. 4 Notwithstanding its rarity, our case reveals the importance of diagnosing this lesion at an early stage because timely decompressive surgery might be beneficial. 5 Familiarity with the anatomy of the vagus, recurrent laryngeal, and phrenic nerves will be helpful in diagnosing the location of the tumor (Figure 2B).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2018R1D1A1B07048778).