
Abstract
Malignant transformation of nasal polyps is extremely rare in cases without background inverted papilloma. Human papillomavirus (HPV) is a sexually transmitted infection believed to be associated with oropharyngeal carcinoma via oro-genital sexual contact. We present a case of focal squamous cell carcinoma in situ that occurred on the surface of nasal polyps and was associated with HPV 51. The patient was successfully treated with endoscopic sinus surgery. Clinicians should be aware of the potential for hidden malignancies, and pathologic assessment of tissue specimens must be performed even in simple nasal polyp cases.
Keywords
Introduction
Nasal polyps are chronic inflammatory growths of the sinonasal mucosa. 1 Unlike inverted papilloma, which is associated with malignancy in approximately 10% of cases, malignant transformation of simple inflammatory nasal polyps is rare.2,3 Recently, the authors encountered a case of focal squamous cell carcinoma (SCC) in situ arising from a nasal polyp without evidence of inverted papilloma. Immunohistochemical staining and real-time polymerase chain reaction (RT-PCR) also demonstrated human papillomavirus (HPV) type 51 infection.
Case Report
A 45-year-old male visited the outpatient clinic at the Department of Otorhinolaryngology – Head and Neck Surgery at a university hospital complaining of bilateral nasal obstruction for several years and aural fullness on the right side. The male had worked as a casino dealer for several years and had a smoking history of 25 pack-years. In addition, he had multiple sexual partners and had a history of excision of genital condyloma several years ago. Anterior rhinoscopic examination found that huge nasal polyps filled the entire nasal cavity and protruded from the right nostril; there was no empty space that could enable endoscopic entry (Figure 1A). To a lesser extent, the polyps also filled the nasal cavity on the left side (Figure 1B). On the tympanic membrane, middle ear effusion was observed on the right side (Figure 1C). Computed tomography with contrast enhancement revealed diffuse bilateral pansinusitis and septal deviation with no evidence of abnormal enhanced lesions (Figure 2).
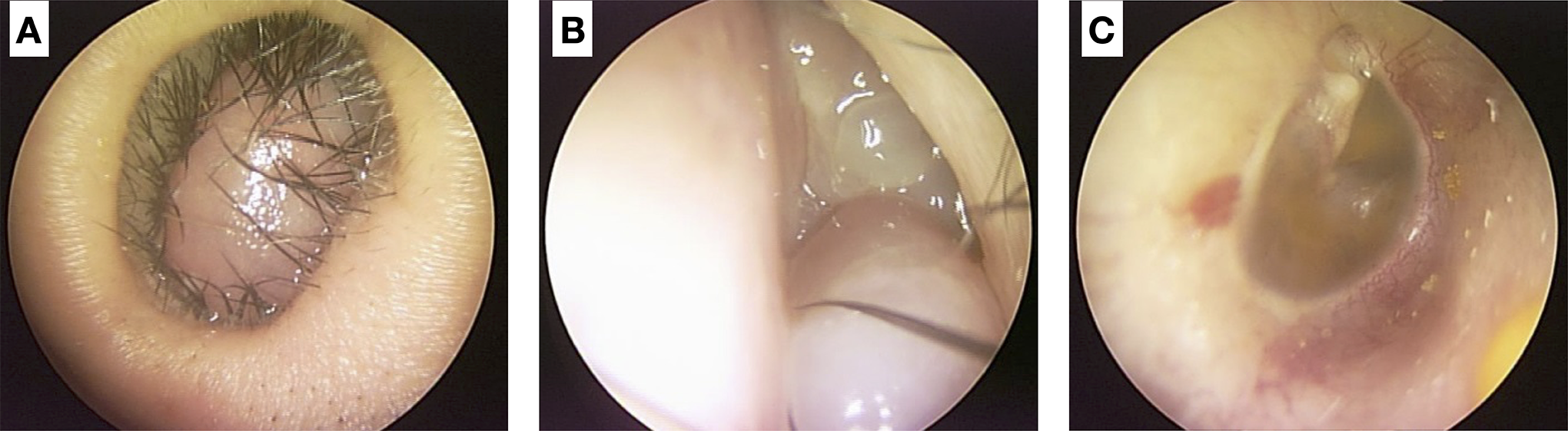
Initial assessment findings. A, Huge nasal polyp filled the entire nasal cavity and protruded from the right nostril. B, Nasal polyp also filled the nasal cavity on the left side. C, Amber-colored tympanic membrane on the right side was observed.
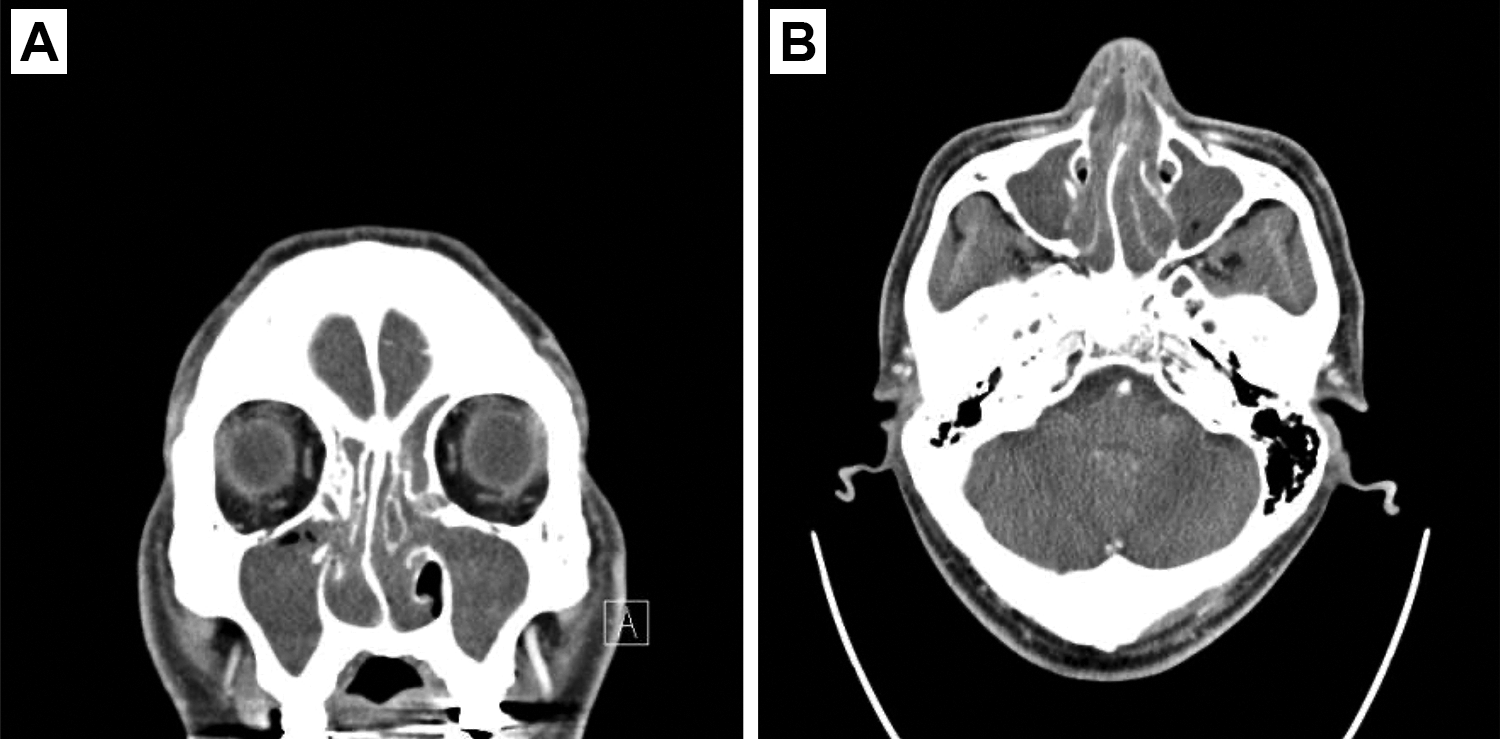
Computed tomography with contrast enhancement revealed diffuse bilateral pansinusitis with no evidence of abnormal enhanced lesions (A, coronal view; B, axial view).
Endoscopic sinus surgery with nasal polypectomy and septoplasty was performed. Polyps were resected as much as possible and sent to the pathologist for evaluation. During the surgery, there were no adverse events except for a considerable amount of bleeding. Tissues obtained were embedded in paraffin blocks and cut into 5-µm sections, then stained with hematoxylin and eosin. The pathology report revealed SCC in situ on the right side and moderate to high-grade dysplasia on the left side against the background of nasal polyps (Figure 3A). The surrounding epithelium showed squamous metaplasia; however, no evidence of inverted papilloma was found. The area of SCC in situ and dysplasia was focal compared to the entire specimen. In addition, perinuclear halos were observed within the dysplastic epithelium, which led us to perform additional immunohistochemical staining and RT-PCR on the suspicion of HPV infection. As a result, strong nuclear and cytoplastic staining for p16 was observed in the same area as that of the SCC in situ (Figure 3B). Additionally, positive staining for Ki-67 (30% positivity; Figure 3C) and p53 (50% positivity; Figure 3D) was observed. Finally, HPV subtype 51 was confirmed by RT-PCR. The patient was discharged from hospital on the second postoperative day without complications. During the postoperative follow-up, additional ventilation tube insertion was performed because of lasting middle ear effusion irrespective of multiple myringotomies. At 1 year after surgery, there was no evidence of SCC recurrence.
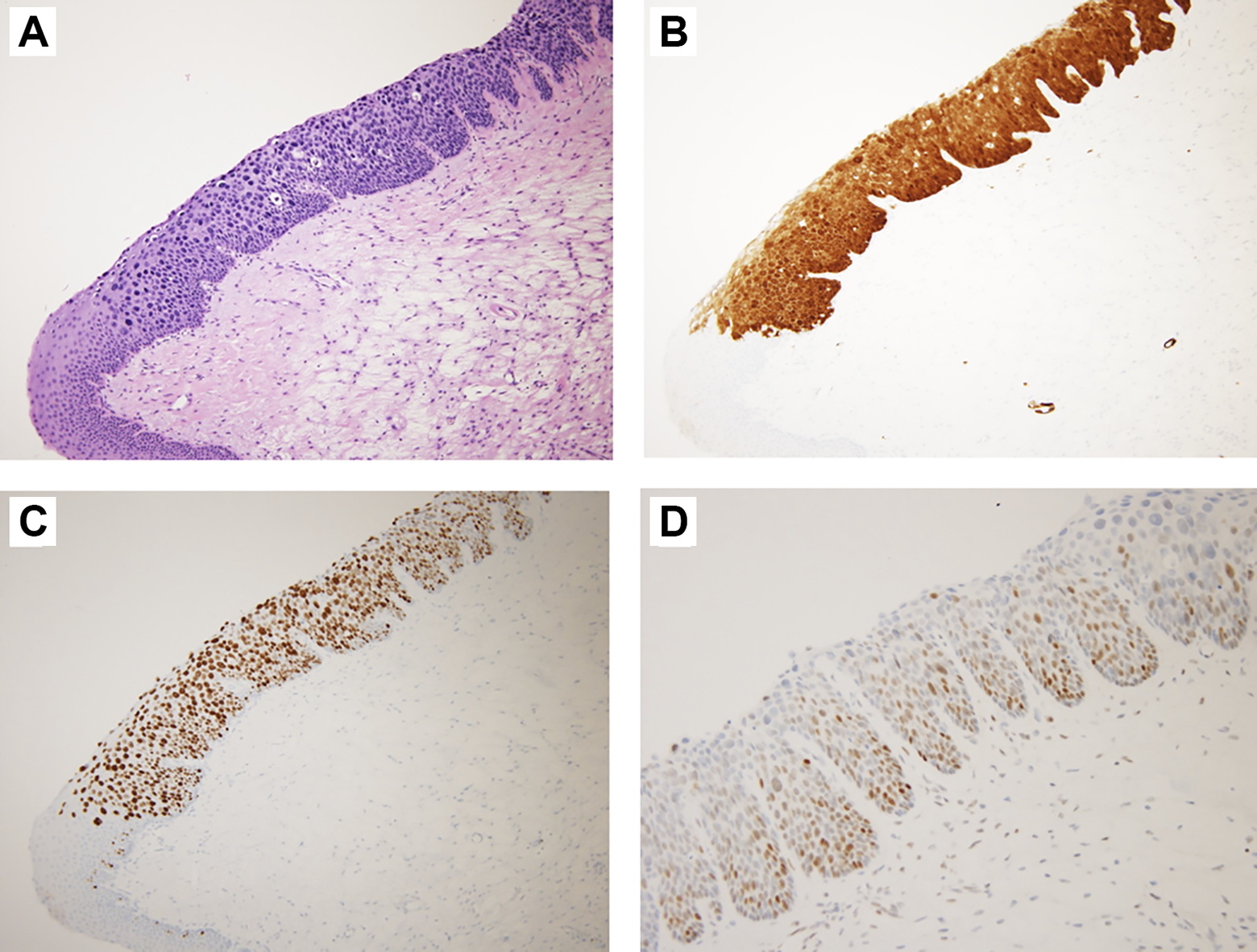
Histopathologic findings of the specimen. A, Hematoxylin and eosin staining (×100) showed squamous cell carcinoma in situ from metaplastic squamous epithelium of a nasal polyp. Perinuclear halos were observed within the dysplastic epithelium. B, p16 staining (×100) showed strong nuclear and cytoplastic staining. C, Ki-67 staining (×100). D, p53 staining (×200).
Discussion
HPV infection is closely related to head and neck SCC (HNSCC) and the overall prevalence of HPV DNA in HNSCC was reported to be 25.9%. 4 Of the HPV types, HPV 16 and 18 are found in almost HPV-positive cancers. 5 To the best of the authors’ knowledge, this is the first report of sinonasal SCC in situ associated with HPV type 51 infection. In addition, malignant transformation of simple nasal polyps is rare in cases without evidence of inverted papilloma.
In general, nasal polyps are covered by pseudostratified columnar epithelium, similar to the lining of other respiratory tracts. However, chronic inflammation such as chronic rhinosinusitis may result in histologic change in the epithelium; that is, squamous metaplasia or erosion. 6 In such cases, significant dysplasia within the epithelium may result from chronic gradual changes followed by squamous metaplasia. In the present case, given that the area of the dysplastic lesion was consistent with the area of positive staining for p16, a surrogate marker for HPV infection, it is evident that HPV infection on the nasal polyps precipitated malignant transformation. 7
Malignant tumors in the sinonasal tract accounts for only 3% of all head and neck cancers and for merely 0.2% of all of carcinomas. 8 Among the various histologic types, though SCC is the most common malignancy of the head and neck area, the sinonasal tract has the lowest fraction of SCC relative to other carcinoma types. 9 In addition, the overall rates of sinonasal SCC have declined over time, making these tumors a complicated and challenging area for clinical practice. 10 The etiology is not fully understood. However, wood dust, chemical substances such as glue and formaldehyde, nickel, and various compounds from the textile industry may be associated with sinonasal SCC. 11 In contrast with most head and neck cancers, smoking increases the risk of sinonasal SCC only 2- to 3-fold. 12 Recently, HPV has been detected in some cases of sinonasal SCC, mainly cases involving malignant transformation of inverted papillomas. 11
HPV is transmitted primarily through sexual contact. Oro-genital contact can lead to oropharyngeal HPV infection and finally oropharyngeal HPV-related SCC. 12 This explains the paradoxical increase of oropharyngeal SCC in spite of the decrease in tobacco-related SCC. 12 In addition to changes in sexual habits, the increased number of sexual partners has also affected HPV infection rates in both the oral cavity and genitalia, leading to HPV becoming an endemic infection. 13 The most common high-risk HPV not only include types 16 and 18 but also include types 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68. 14 An epidemiologic study using high-risk HPV DNA types 16, 18, 31, and 33 demonstrated that 21% of sinonasal carcinoma cases were positive for high-risk HPV, and this HPV infection may act as an oncologic agent. 7 For the patient in the current report, the route of HPV transmission remains unclear. The most plausible hypothesis is that it was transmitted from the genitals to the sinonasal tract because the nasal polyps were protruding from his nostrils. In addition, his previous history of genital condyloma strongly supports this hypothesis. While the detailed orientation of the lesion remains unknown, the surface of the nasal polyps protruding from the nostril might be the lesion site.
On the other hand, routine histopathologic analysis for nasal polyps is controversial. Some advocate routine evaluation by providing examples of hidden malignancy. 15 Others oppose routine evaluation because the detection rate is low (below 1%) and the cost is high. 16 In the current case, obtaining sufficient biopsy material and carrying out a diverse diagnostic workup could prevent misdiagnosis.
In conclusion, we encountered focal SCC in situ arising from simple nasal polyps and associated with HPV 51. Clinicians should keep in mind that hidden malignancies are always possible, and pathologic evaluation of all tissue specimens should be carried out even in simple nasal polyp cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.