
Abstract

A 13-month-old boy was referred to the emergency department from the pediatrician’s office for increased shortness of breath. A 2-view chest X-ray was ordered revealing right hemithorax hyperlucency, minimal lung markings, and leftward mediastinal shift (Figure 1). ENT was consulted for possible airway foreign body. On examination, the child was well appearing without stridor or noisy breathing. Lung auscultation revealed decreased breath sounds on the right; a right chest wall prominence was noted. The parents reported a history of progressively worsening dyspnea over the previous 4 weeks but no witnessed foreign body aspiration, cough, wheeze, or fevers. His clinical history did not clearly support an airway foreign body. Computed tomography thorax with contrast was recommended and demonstrated an 11.5 × 11.8 × 8.1 cm multilocular cystic lesion in the right upper/middle pulmonary lobe causing a leftward mediastinal shift (Figure 2). Differential diagnosis at this point was congenital pulmonary airway malformation (CPAM) versus pleuropulmonary blastoma. The next day, he underwent a right thoracotomy with right middle lobe resection and chest tube placement. He was discharged on postoperative day 4 without complication and with improved lung function. The final pathologic specimen demonstrated a CPAM type IV.

Chest X-ray demonstrating right hemithorax hyperlucency, minimal lung markings, and leftward mediastinal shift.
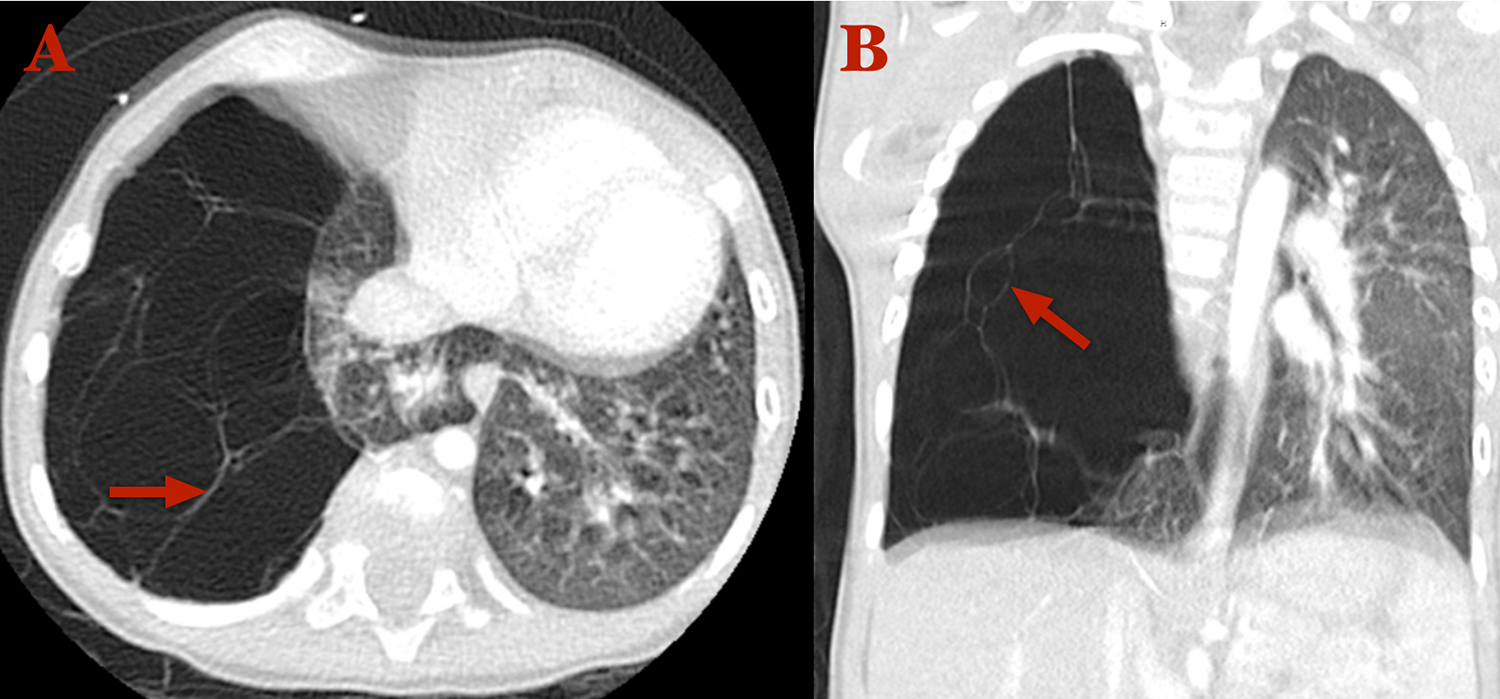
Computed tomography (CT) thorax with contrast in axial (A) and coronal (B) windows revealing a large multilocular cystic pulmonary lesion in the right upper/middle pulmonary lobe with multiple thin septations (arrows), marked left mediastinal shift, and substantial volume loss.
First described by Ch’in and Tang in 1949, CPAM is a rare developmental anomaly that replaces lung tissue with nonfunctioning cystic tissue. 1 Congenital pulmonary airway malformations account for 95% of a group of pathologies referred to as congenital cystic lung lesions (CCLLs), and they are the most common developmental congenital anomaly of the lung. 2 Previous population-based studies have estimated their incidence at 1 in 25 000 to 1 in 35 000 pregnancies. 3 However, with advancements in ultrasonography, their incidence continues to increase and could be as high as 1 in 3000 pregnancies.4,5 In 2016, Hardee et al found 85% of CCLLs were correctly diagnosed via prenatal ultrasound, consistent with the estimated sensitivity, and specificity of prenatal ultrasound of 90% and 77%, respectively.6,7 In our case, the patient’s mother reported a normal prenatal ultrasound and noncomplicated pregnancy.
The clinical presentation of a CPAM varies widely including an asymptomatic appearance, recurrent respiratory infections, and/or severe respiratory distress. 8 Given only 30% to 40% of patients with CPAM are symptomatic in the neonatal period, it has been a challenge for clinicians to correctly diagnose CPAM on symptoms alone.9,10 Reliance on chest x-ray often leads to misdiagnosis given its 61% sensitivity. 11 Congenital pulmonary airway malformation has been misdiagnosed as pneumonia, congenital diaphragmatic hernia, pneumatocele, tuberculosis, and pneumothorax—often leading to inappropriate chest tube placement.12-14
More commonly encountered, pediatric foreign body aspiration is a potentially life-threatening emergency and leading cause of morbidity in children less than 1 year old.15,16 In 2000 alone, over 17 000 emergency visits in children younger than 14 years were attributed to foreign body inhalation. 15 The most common presenting signs and symptoms include new-onset cough (88%), choking/gagging (67%), wheezing (57%), stridor/noisy breathing (41%), dyspnea (20%), and for children with a delayed presentation ≥7 days after foreign body aspiration, fever (53%). 17 The most common radiographic findings in patients were air trapping/hyperinflation (33%) and atelectasis (16%). 17 A review of the literature suggests varying diagnostic value of the aforementioned clinical and radiographic findings. A history of coughing has a high sensitivity (73.7%-88%) but poor specificity (18%-35%).17-21 The sensitivity and specificity of unilaterally decreased breath sounds seems to be more variable ranging from 41% to 80% and 42.3% to 91%, respectively.17-19,21-23 Physical examination has a sensitivity of 70.5% to 90% and a specificity of 26% to 63%.17,21,24-26 The sensitivity and specificity of chest radiography varies from 61% to 88% and 30% to 77%, respectively.17,19-21,24-27 Perhaps the most specific finding, air trapping on chest x-ray has reported sensitivity and specificity of 33% to 79% and 66.7% to 97.4%, suggesting it is far from an ideal diagnostic indicator.17,18,21-23,28 To this day, endoscopic evaluation remains the definitive method to diagnose and remove an inhaled foreign body.29,30
Deciding if a patient is an operative candidate for a rigid bronchoscopy can be a difficult decision and requires a good history, physical examination, and in many cases, radiographic imaging. When the index of suspicion of foreign body aspiration is high, expeditiously proceeding with bronchoscopy is crucial. However, when the clinical picture doesn’t quite fit, as was the case with this patient, it is also important to review one’s differential diagnosis. Bronchial compression, plastic bronchitis, and CPAM are among the numerous pathologies that resemble bronchial obstructing foreign bodies. 31 As otolaryngologists, we should always have a high suspicion and low threshold to perform a rigid bronchoscopy if a foreign body aspiration is suspected. Equally important is our role to remember our differential diagnosis in order to minimize risk and provide patients with the best, most well-informed care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.