
Abstract
Background:
Laser irradiation of the semicircular canal (SCC) is a good treatment for intractable benign paroxysmal positional vertigo. However, there were few reports on the temperature changes during laser irradiation.
Objective:
To measure the internal temperature of the SCC and vestibule during green laser irradiation of the SCC and investigate morphologic changes using human temporal bones.
Methods:
After the lateral SCC was blue-lined, a thermocouple was inserted into the SCC through a hole made in the canal wall. Another thermocouple was inserted into the vestibule through the oval window. Green laser was irradiated to the lateral canal wall. After the irradiation, the tissues were inspected as paraffin using HE staining.
Result:
The internal temperature of the SCC rose from 33 ° to 52 °C by a single laser irradiation of 1.5 W × 2 seconds and 82 °C by a single laser irradiation of 1.7 W × 3 seconds to the canal wall with a black spot. Continuous laser irradiation of 1.5 W × 3 seconds, 10 times resulted in a temperature rise of 92 °C from 33 °C. Throughout the whole experiments, temperatures within the vestibule were unchanged. Histopathology showed that the irradiated areas of the lateral canal wall were partially deficient with or without carbonization after single irradiation. By continuous laser irradiations, the SCC bony wall showed a peroration of 40 µm in diameter with carbonized edges.
Conclusions:
Green laser irradiation of the SCC produced char formation with perforation in the canal wall. High temperatures within the SCC were recorded for a short period of less than 30 seconds. However, the vestibule didn’t show temperature changes.
Keywords
Introduction
Benign paroxysmal positional vertigo (BPPV) is one of the most common peripheral vestibular disorders. Free-floating endolymph particles (otoconia) displaced from the utricle gravitate into the posterior semicircular canal and make this canal sensitive to gravity. 1 Most patients will be successfully treated with canalith repositioning maneuvers. However, sometimes we encounter patients with recurrences and intractable cases. Surgical interventions such as singular neurectomy, 2 canal plugging, 3 -5 and laser irradiation 6 are required treatments.
We performed a series of experiments using argon laser irradiation of the inner ear, particularly to the otolithic organs, 7 -10 as well as semicircular canals. 11 -13 Laser irradiation of the semicircular canal resulted in char formation of the bony canal wall and constriction of the semicircular duct. Fibrosis then developed within the canal, followed by ossification. Movement of the endolymph is probably restricted within the irradiated canal. Our surgical method using laser irradiation does not need opening of the semicircular canal. 14,15 As the semicircular duct adheres to the outer wall of the bony canal, heat produced on the canal wall will constrict the semicircular duct, resulting in restriction of the endolymph movement. In animal experiments, no changes were observed in the ABR measurements after the appropriate irradiation of the semicircular canal. 12 However, to our knowledge, no experimental studies have been reported on the temperature changes inside the semicircular canal and vestibule during laser irradiation. The purpose of this study was to measure the inside temperature of the semicircular canal and vestibule during laser irradiation of the semicircular canal using human temporal bones.
Material and Methods
Archival temporal bones removed at autopsy and fixed in 10% formalin solution were used in these experiments. Instead of the posterior semicircular canal, the lateral semicircular canal was selected as the target of green laser irradiation for the convenience of performing the experimental procedures. Type K (chromel–alumel) thermocouples were used for measurement of the temperature accurately and its range is from −200 °C to +1350 °C. Chromel is an alloy mainly made of nickel. Alumel is an alloy mainly composed of nickel and chromium. In this experiment, we prepared a thermocouple with a diameter of 0.08 mm to be inserted into the semicircular canal and another with a 0.5 mm diameter into the vestibule.
After a mastoidectomy, the lateral semicircular canal was blue-lined for a distance of 3 mm. A small hole was then created in the distal portion of the blue-lined area for insertion of the thermocouple. Another thermocouple was placed within the vestibule after removing the stapes (Figure 1). Each temporal bone block was placed on a laboratory dish with warm water (37 °C ). Half of the block was soaked in the water during the experiments. Care was taken to prevent the warm water reaching the labyrinth.
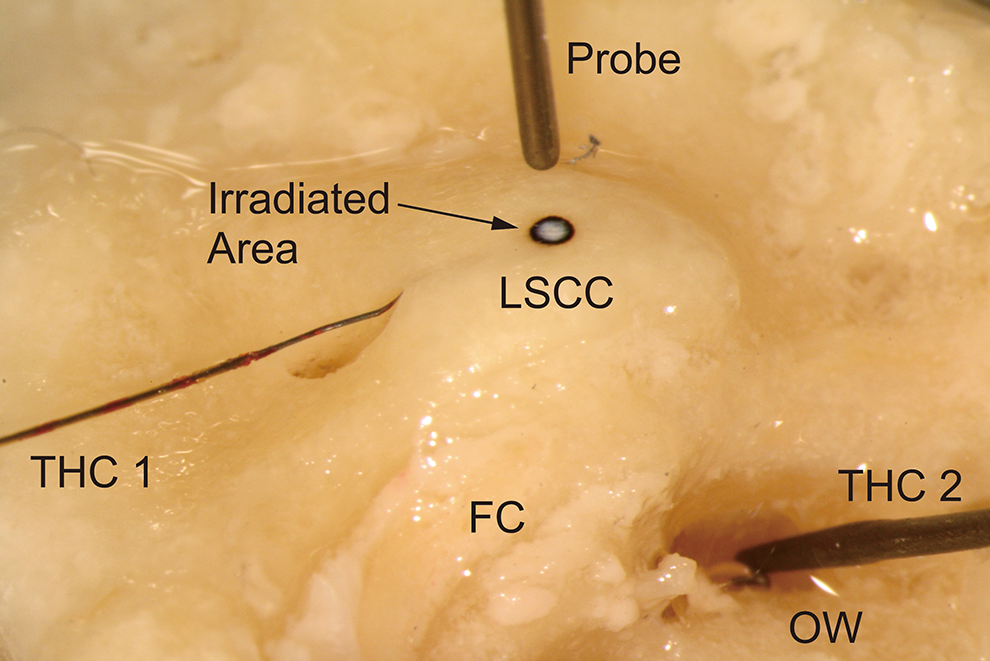
Temporal bone after consecutive irradiations of 1.5 W × 3 seconds, 10 times. Laser probe, thermocouples, and burned area of the right human temporal bone. The irradiated area shows a carbonized circle with a perforation at the center. THC 1: A 0.08 mm diameter thermocouple was inserted into the lateral semicircular canal. THC 2: A 0.5 mm diameter thermocouple was placed into the vestibule. FC indicates facial canal; LSCC, lateral semicircular canal; OW, oval window.
The wavelength of the green laser was close to that of argon laser, 532 nm. A laser probe with a diameter of 300 µm was connected to a green laser system (GTC-1000; NIDEC Co). The tip of the laser probe was directed perpendicular to the target on the surface of the blue-lined canal wall. The distance between the probe tip and target was about 2 mm.
Laser irradiation was performed under the following 3 conditions—(1) single laser irradiation: 1.5 W power was applied on the dial of the device for 2 seconds; (2) consecutive laser irradiations: 1.5 W power was applied on the dial of the device for 3 seconds for 10 consecutive times; and (3) single laser irradiation to a black mark on the blue line: 1.7 W power was applied on the dial of the device for 3 seconds and 1 time. The black mark was painted on the canal wall to direct the irradiation.
After the irradiation, the temporal bones were decalcified with KalkitoxTM (Wako Pure Chemical Industries, Ltd), embedded in paraffin and sectioned perpendicular to the lateral semicircular canal at a thickness of 10 µm. Sections were stained with hematoxylin and eosin.
The cadavers were donated with the individual’s consent. The research was conducted in accordance with Article 18 of the Cadaver, Autopsy, and Preservation Act. This study was approved by the institutional review board of Showa University School of Medicine.
Results
A single laser irradiation (1.5 W × 2 seconds, 1 time).
The internal temperature of the semicircular canal increased from 33 °C to 52 °C by laser irradiation, and it returned to 33 °C after about 20 seconds. The temperature of the vestibule was not changed (Figure 2A). Histopathologically, the bone of the semicircular canal was partially deficient without carbonization.
Consecutive laser irradiation (1.5 W × 3 seconds, 10 times).
The internal temperature of the semicircular canal increased from 33 °C to 70 °C at the first irradiation, and when the irradiation was applied 10 times consecutively, the temperature increased to 92 °C. The temperature returned to 33 °C 60 seconds after cessation of the irradiation. The temperature of the vestibule was unchanged (Figure 2B). Histopathologically, the semicircular canal wall was partially deficient and carbonized. The endosteum was unchanged (Figures 1 and 2C).
A single laser irradiation of the blue-lined canal wall with a black spot (1.7 W × 3 seconds, 1 time).
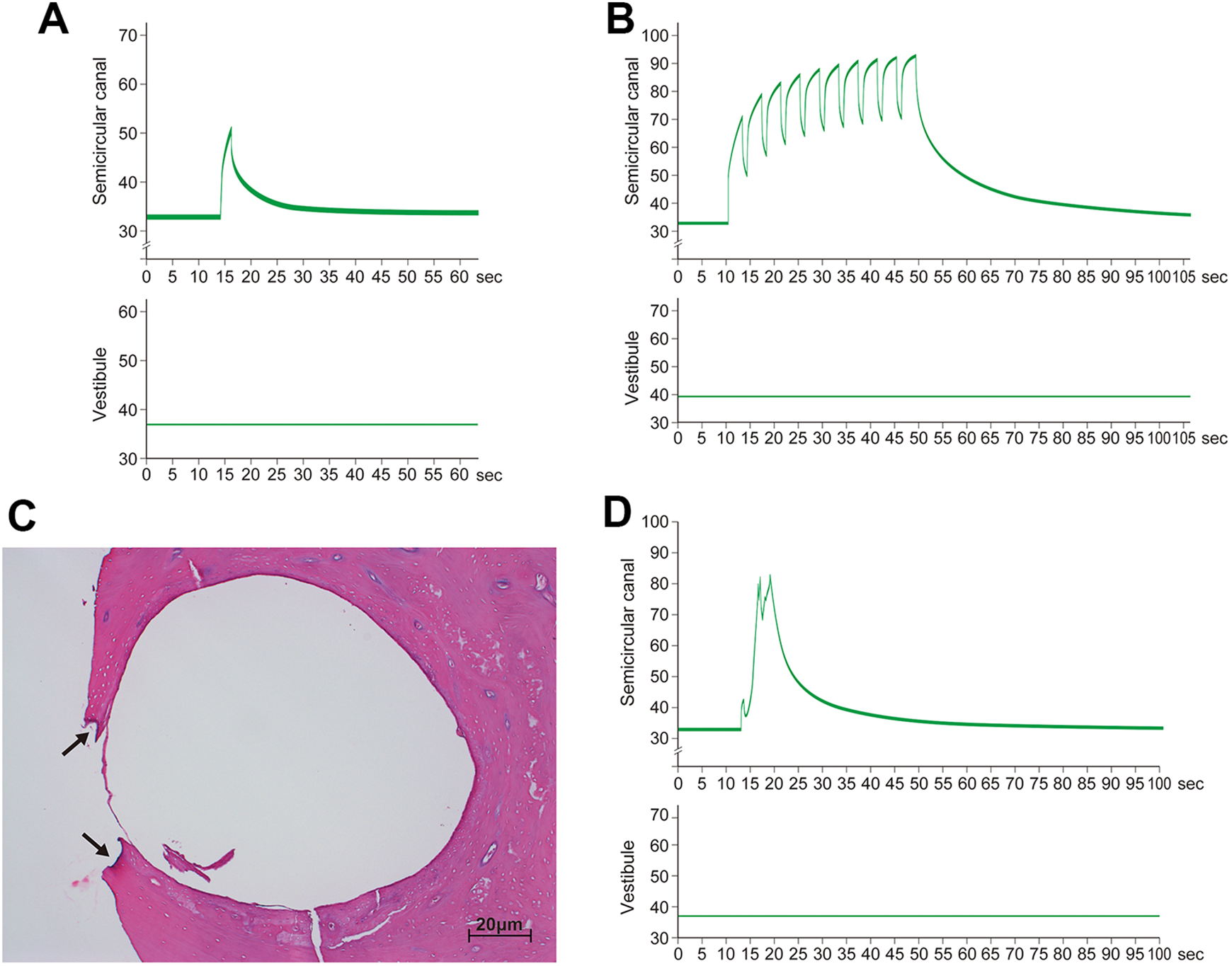
Changes in temperature in the LSCC and vestibule during laser irradiation. A, A single irradiation of 1.5 W × 2 seconds. The upper figure: The temperature changes from 33 °C to 50 °C, which returns to the pre-irradiation value in 20 seconds. The lower figure: No changes observed in the vestibule. B, Consecutive irradiations of 1.5 W × 3 seconds, 10 times The upper figure: The temperature increases each time, starting from 33 °C to 70 °C, and to 92 °C at the 10th irradiation. The temperature returns to the pre-irradiation level in 60 seconds. The lower figure: No temperature changes in the vestibule. C, Histology showing a bony wall defect and carbonized edges (arrows) after 10 consecutive irradiations (each time 1.5 W × 3 seconds). The endosteum was unchanged. The semicircular duct cannot be evaluated. Specimen with a 10-µm thickness and H & E staining. D, Single irradiation of 1.7 W × 3 seconds. The upper figure: The temperature in the canal increases from 33 °C to 82 °C. The temperature returns to the previous level in 20 seconds. The lower figure: No temperature changes observed in the vestibule. LSCC indicates lateral semicircular canal.
The internal temperature of the semicircular canal increased from 33 °C to 82 °C by laser irradiation and returned to 33 °C 30 seconds after the cessation. The temperature of the vestibule was unchanged (Figure 2D). Histopathologically, the irradiated area of the semicircular canal wall was partially deficient without carbonization.
Discussion
As BPPV is a benign disease, surgery should only be reserved for the most intractable or recurrent cases. 16 Most cases with BPPV can be treated without surgical procedures. The intractable case we reported was unable to walk because of severe vertigo with nystagmus. We found difficulty in performing positional and positioning nystagmus tests because the patient could not keep her eyes open. However, we confirmed the lateral and posterior canals were responsible for vertigo of the patient.
Prokopakis et al 17 evaluated 592 patients prospectively and the mean follow-up was 46 months. Symptoms were relieved immediately after the first canalith repositioning procedure in 497 (84%) patients. Seventy-two (12%) patients reported recurrence and the mean time to recurrence was 26 months. Considering the above, it is estimated that less than 1% of cases with BPPV require surgery. However, the prevalence of BPPV has been reported to be 107 cases per 100 000 population per year, 18 so the number of cases requiring surgery is likely to be significant.
Surgical therapy has been well described for posterior semicircular canal BPPV and is quite successful at relieving symptoms. 19 The concept of posterior semicircular canal occlusion for BPPV 3 -5 is that the obstruction of the semicircular canal lumen prevents endolymph flow. This effectively fixes the cupula and renders it unresponsive to normal angular acceleration forces and stimulation from either free-floating particles within the endolymph or a fixed cupular deposit.
One of the present authors reported that a patient with severe traumatic BPPV was successfully treated with argon laser irradiation of the posterior and lateral semicircular canals. 15 The patient was free from vertigo on the 2nd postoperative day throughout her life for 16 years until her death. The concept of laser irradiation of the semicircular canal is similar to semicircular canal occlusion. Heat produced on the canal wall will constrict the semicircular duct, resulting in restricted endolymph movement. 11 -13 The effects of heat on the cochlea were unknown in this patient because the patient had already lost her hearing due to ear trauma. However, in animals to which argon laser was applied to the semicircular canals, the cochlea was normal. 12 The irradiated semicircular canal exhibited marked constriction of the semicircular duct, disintegration of its epithelial cell layer, and fibrosis within the canal followed by ossification. The patient’s computed tomography 16 years after the surgery showed that the argon laser irradiation to the blue-lined semicircular canals did not occlude the canal of the corresponding areas. 15 The size of the human semicircular canal is larger than that of a guinea pig, and the applied power of the laser irradiation is likely insufficient to cause ossification of the human semicircular canal. During laser irradiation, splashing of a small amount of inner ear fluid from the target area was observed, which is indicative of the transmission of the high temperature from the burning canal wall to the inner ear fluids. Perhaps, the constriction of the semicircular duct occurred concomitantly. Immediate relief of her vertigo after the irradiation is likely due to constriction of the semicircular duct.
The present study revealed that the temperature inside the semicircular canal increased for 20 to 30 seconds under a single laser irradiation of 1.5 to 1.7 W for 2 to 3 seconds. Heat produced by laser irradiation does not reach the vestibule or cochlea. Splashing of the inner ear fluid probably minimizes the temperature increase of the inner ear. Char formation and fluid splashing are indications of canal bone burning and semicircular duct constriction. In practice, the target semicircular canal should be irradiated consecutively in order to obtain complete constriction of the canal. A pause of 30 seconds between each irradiation is imperative (Figure 3).
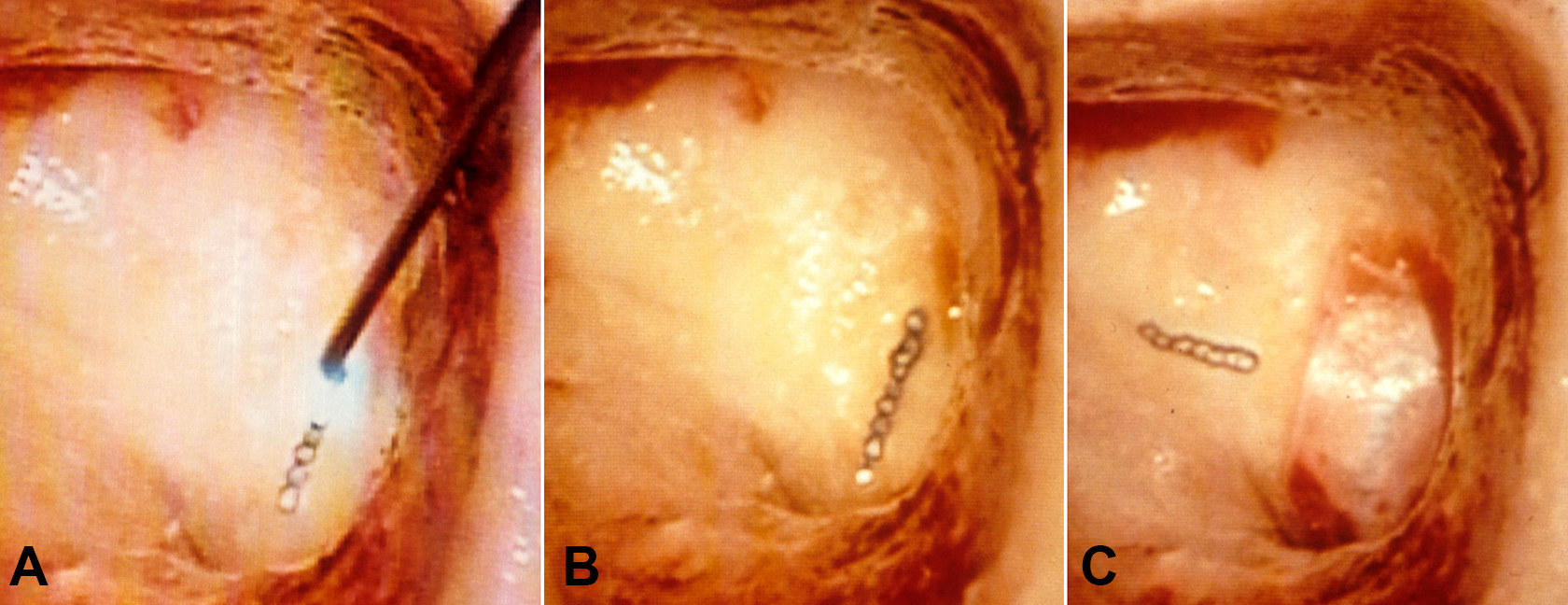
Irradiating semicircular canals. 14 A, After mastoidectomy of the left ear, the lateral and posterior semicircular canals were blue-lined. The posterior canal was consecutively irradiated by an argon laser beam along the blue line for 3 mm. A 1.5 W power was applied each time for 3 seconds. The blue line of the lateral canal was not clear in the photograph. B, Irradiation of the posterior canal completed. C, The irradiated posterior canal was covered by a sheet of fascia. The lateral canal was irradiated by the argon laser 7 times. Intervals of 30 seconds are essential between irradiations to prevent overheating of the labyrinth.
Argon laser irradiation of 1.5 W × 0.5 second produced a black spot (carbonization) and a small amount of heated inner ear fluid immediately appeared around the black spot, 14,15 which indicates bony dehiscence. The presence of deficiencies in the canal wall are probably indication of vaporization, even if carbonization was not be observed. A black mark on the canal wall make it easy to render the tissue carbonized.
Surgical methods for BPPV are either canal plugging or singular neurectomy. The surgical procedures we performed were blue-lining the canal wall, laser irradiation, and covering the irradiated area with a piece of fascia. As the procedures don’t require opening the canal wall and the present study shows no heat effect on the cochlea, the laser irradiation method seems to be superb.
Conclusion
We measured changes of the internal temperature of the lateral semicircular canal and vestibule during laser irradiation of the semicircular canal of human temporal bones. Green laser was used in this series of experiments to irradiate the lateral semicircular canal wall. Powers of 1.5 and 1.7 W were applied to the lateral canal for 2 and 3 seconds. After a single irradiation, the internal temperature increased from 33 °C to 52 °C, and 33 °C to 70 °C, respectively. The temperature returned to the previous value in 30 seconds. Ten consecutive irradiations (1.5 W, 3 seconds) resulted in a high temperature increase from 33 °C to 92 °C. The temperature returned to 33 °C in 60 seconds. No temperature increase was observed in the vestibules of the irradiated bones. The irradiated canal wall showed the formation of a bony defect with/without char formation of the edges.
A single irradiation of green laser to the canal wall was able to create a small burn on the canal wall without influencing the cochlea. In the cases where repeated irradiation are required, a pause of 30 seconds is recommended. Application of a green laser to the lateral canal showed no influence on the cochlea with regard to heat transmission.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI Grant Number JP24592561.