
Abstract
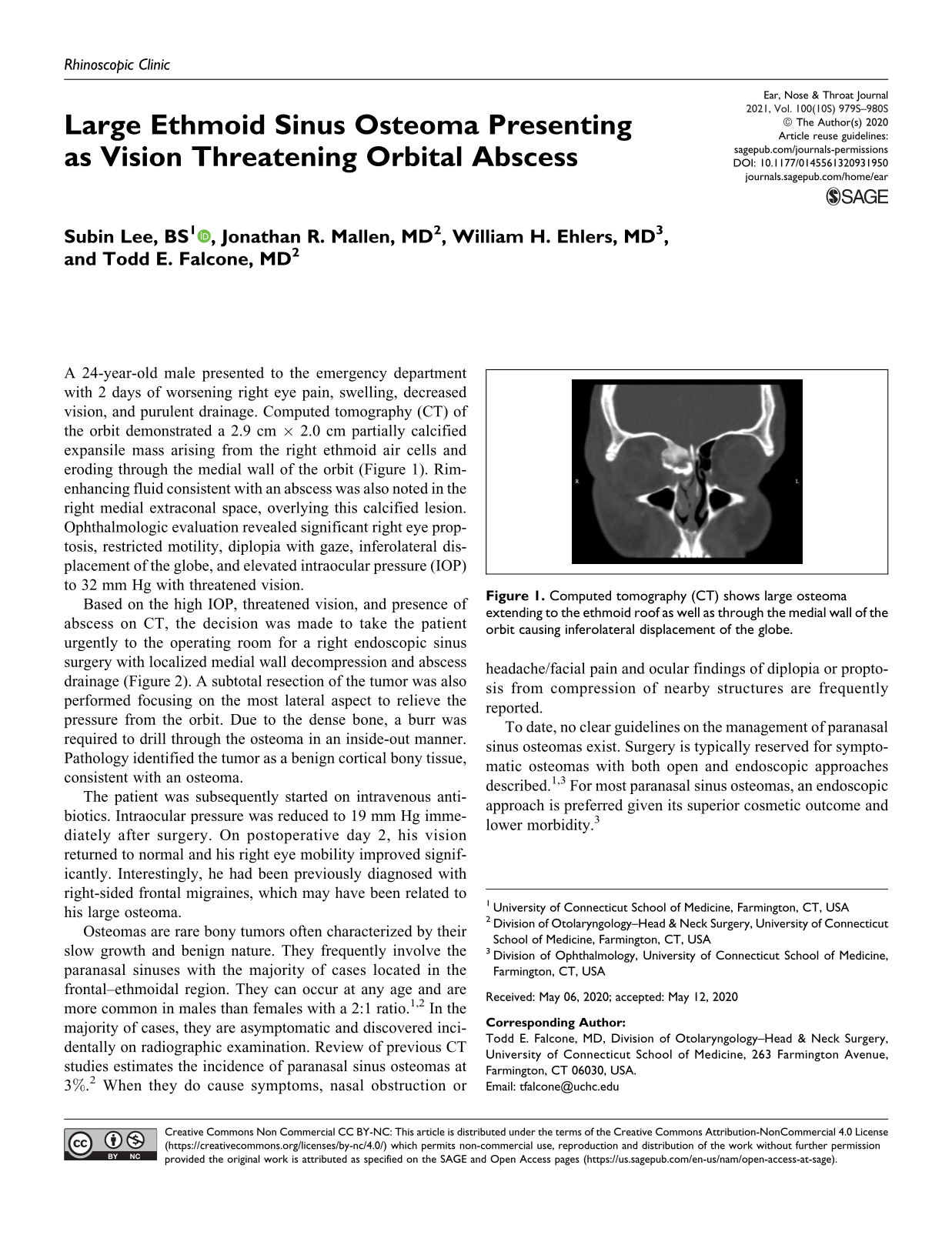
A 24-year-old male presented to the emergency department with 2 days of worsening right eye pain, swelling, decreased vision, and purulent drainage. Computed tomography (CT) of the orbit demonstrated a 2.9 cm × 2.0 cm partially calcified expansile mass arising from the right ethmoid air cells and eroding through the medial wall of the orbit (Figure 1). Rim-enhancing fluid consistent with an abscess was also noted in the right medial extraconal space, overlying this calcified lesion. Ophthalmologic evaluation revealed significant right eye proptosis, restricted motility, diplopia with gaze, inferolateral displacement of the globe, and elevated intraocular pressure (IOP) to 32 mm Hg with threatened vision.

Computed tomography (CT) shows large osteoma extending to the ethmoid roof as well as through the medial wall of the orbit causing inferolateral displacement of the globe.
Based on the high IOP, threatened vision, and presence of abscess on CT, the decision was made to take the patient urgently to the operating room for a right endoscopic sinus surgery with localized medial wall decompression and abscess drainage (Figure 2). A subtotal resection of the tumor was also performed focusing on the most lateral aspect to relieve the pressure from the orbit. Due to the dense bone, a burr was required to drill through the osteoma in an inside-out manner. Pathology identified the tumor as a benign cortical bony tissue, consistent with an osteoma.
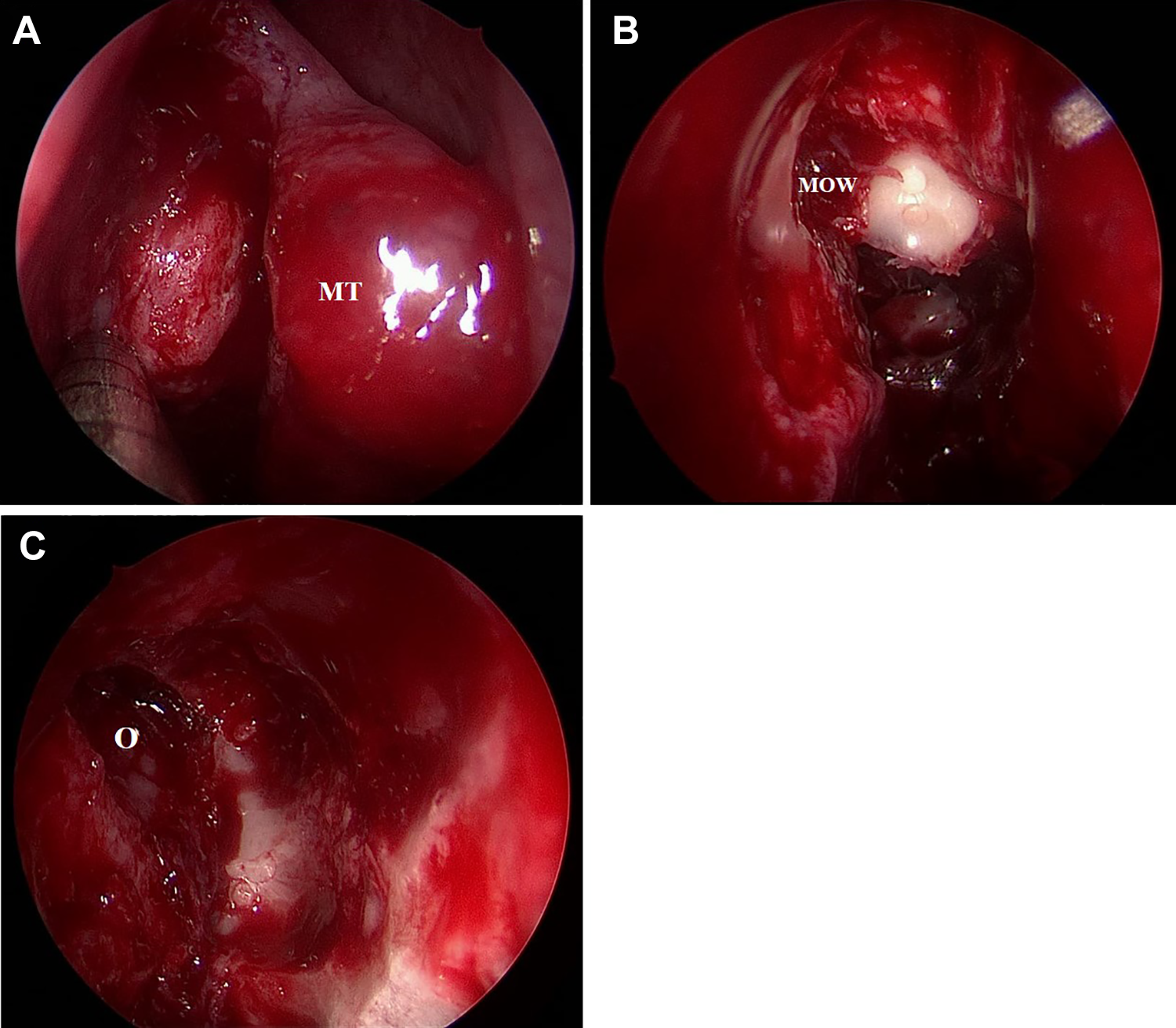
Osteoma located in anterior ethmoid sinus (A). View of medial orbital wall and dense bone of osteoma (B). Orbit following removal of osteoma and lamina papyracea (C). MOW indicates medial orbital wall; MT, middle turbinate; O, orbit.
The patient was subsequently started on intravenous antibiotics. Intraocular pressure was reduced to 19 mm Hg immediately after surgery. On postoperative day 2, his vision returned to normal and his right eye mobility improved significantly. Interestingly, he had been previously diagnosed with right-sided frontal migraines, which may have been related to his large osteoma.
Osteomas are rare bony tumors often characterized by their slow growth and benign nature. They frequently involve the paranasal sinuses with the majority of cases located in the frontal–ethmoidal region. They can occur at any age and are more common in males than females with a 2:1 ratio.1,2 In the majority of cases, they are asymptomatic and discovered incidentally on radiographic examination. Review of previous CT studies estimates the incidence of paranasal sinus osteomas at 3%. 2 When they do cause symptoms, nasal obstruction or headache/facial pain and ocular findings of diplopia or proptosis from compression of nearby structures are frequently reported.
To date, no clear guidelines on the management of paranasal sinus osteomas exist. Surgery is typically reserved for symptomatic osteomas with both open and endoscopic approaches described.1,3 For most paranasal sinus osteomas, an endoscopic approach is preferred given its superior cosmetic outcome and lower morbidity. 3
Our case is unusual and novel in 2 respects. First, the size of the osteoma is notable, nearly approaching the cutoff of a giant osteoma (>3.0 cm). Second, the significant orbital extension of this osteoma leads to substantial inferolateral displacement of the globe and ultimately, an orbital abscess with increased IOP, threatening the patient’s vision. This is a rare occurrence as the incidence of intraorbital complications from an osteoma is estimated at only 0.9% to 5.1% of all orbital tumors.1,2
As our case highlighted, an urgent endoscopic approach to orbital decompression and ethmoid osteoma resection was used to successfully treat an orbital abscess. At 2-month follow-up, the patient continues to be asymptomatic. There are ongoing discussions regarding complete osteoma resection to avoid recurrence, frontal sinusitis, and further treat his underlying headache disorder although there are conflicting reports on the recurrence of incompletely removed osteomas. 4
Footnotes
Authors’ Note
Submitted for poster presentation at the Academy of Otolaryngology–Head & Neck Surgery Annual Meeting; September 13-16, 2020; Boston, MA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.